Learn about the nursing care management of patients with asthma in this nursing study guide .

Table of Contents
- What is Asthma?
Pathophysiology
- Statistics and Epidemiology
Clinical Manifestations
Complications, assessment and diagnostic findings, pharmacologic therapy, peak flow monitoring, nursing assessment, nursing diagnosis, nursing care planning & goals, nursing interventions, discharge and home care guidelines, documentation guidelines, what is asthma.
Asthma affects people in their different stages in life, yet it can be avoided and treated.

- Asthma is a chronic inflammatory disease of the airways that causes airway hyperresponsiveness, mucosal edema , and mucus production.
- Inflammation ultimately leads to recurrent episodes of asthma symptoms.
- Patients with asthma may experience symptom-free periods alternating with acute exacerbations that last from minutes to hours or days.
- Asthma, the most common chronic disease of childhood, can begin at any age.
The underlying pathophysiology in asthma is reversible and diffuse airway inflammation that leads to airway narrowing.
- Activation. When the mast cells are activated, it releases several chemicals called mediators.
- Perpetuation. These chemicals perpetuate the inflammatory response, causing increased blood flow, vasoconstriction,, fluid leak from the vasculature, the attraction of white blood cells to the area, and bronchoconstriction.
- Bronchoconstriction. Acute bronchoconstriction due to allergens results from a release of mediators from mast cells that directly contract the airway.
- Progression. As asthma becomes more persistent, the inflammation progresses and other factors may be involved in the airflow limitation.
Statistics and Epidemiology
Asthma is considered the most common chronic disease of childhood and is a disruptive disease that affects school and work attendance.
- Asthma affects more than 22 million people in the United States.
- Asthma accounts for more than 497, 000 hospitalizations annually.
- The total economic cost of asthma exceeds $27.6 billion.
Despite increased knowledge on the pathology of asthma and the development of improved medications and management plans, the death rate from the disease continues to rise. Here are some of the factors that influence the development of asthma.
- Allergy . Allergy is the strongest predisposing factor for asthma.
- Chronic exposure to airway irritants. Irritants can be seasonal (grass, tree, and weed pollens) or perennial (mold, dust, roaches, animal dander).
- Exercise. Too much exercise can also cause asthma.
- Stress/ Emotional upset. This can trigger constriction of the airway leading to asthma.
- Medications. Certain medications can trigger asthma.
The signs and symptoms of asthma can be easily identified, so once the following symptoms are observed, a visit to the physician is necessary.
- Most common symptoms of asthma are cough (with or without mucus production), dyspnea , and wheezing (first on expiration , then possibly during inspiration as well).
- Cough . There are instances that cough is the only symptom.
- Dyspnea. General tightness may occur which leads to dyspnea .
- Wheezing. There may be wheezing, first on expiration, and then possibly during inspiration as well.
- Asthma attacks frequently occur at night or in the early morning.
- An asthma exacerbation is frequently preceded by increasing symptoms over days, but it may begin abruptly.
- Expiration requires effort and becomes prolonged.
- As exacerbation progresses, central cyanosis secondary to severe hypoxia may occur.
- Additional symptoms, such as diaphoresis, tachycardia, and a widened pulse pressure, may occur.
- Exercise-induced asthma: maximal symptoms during exercise, absence of nocturnal symptoms, and sometimes only a description of a “choking” sensation during exercise.
- A severe, continuous reaction, status asthmaticus, may occur. It is life-threatening.
- Eczema, rashes, and temporary edema are allergic reactions that may be noted with asthma.
Patients with recurrent asthma should undergo tests to identify the substances that precipitate the symptoms.
- Allergens . Allergens, either seasonal or perennial, can be prevented through avoiding contact with them whenever possible.
- Knowledge. Knowledge is the key to quality asthma care.
- Evaluation. Evaluation of impairment and risk are key in the control.
Complications for asthma include the following:
- Status asthmaticus . Airway obstruction in status asthmaticus often results in hypoxemia .
- Respiratory failure . Asthma, if left untreated, progresses to respiratory failure.
- Pneumonia . Mucus that pools in the lungs and becomes infected can lead to the development of pneumonia .
To determine the diagnosis of asthma, the clinician must determine that episodic symptoms of airway obstruction are present.
- Positive family history . Asthma is a hereditary disease, and can be possibly acquired by any member of the family who has asthma within their clan.
- Environmental factors . Seasonal changes, high pollen counts, mold, pet dander, climate changes, and air pollution are primarily associated with asthma.
- Comorbid conditions . Comorbid conditions that may accompany asthma may include gastroeasophageal reflux, drug-induced asthma, and allergic broncopulmonary aspergillosis.
Medical Management
Immediate intervention may be necessary, because continuing and progressive dyspnea leads to increased anxiety , aggravating the situation.
- Short-acting beta 2 – adrenergic agonists . These are the medications of choice for relief of acute symptoms and prevention of exercise-induced asthma.
- Anticholinergics . Anticholinergics inhibit muscarinic cholinergic receptors and reduce intrinsic vagal tone of the airway.
- Corticosteroids. Corticosteroids are most effective in alleviating symptoms, improving airway function, and decreasing peak flow variability.
- Leukotriene modifiers. Anti Leukotrienes are potent bronchoconstrictors that also dilate blood vessels and alter permeability.
- Immunomodulators . Prevent binding of IgE to the high affinity receptors of basophils and mast cells.

- Peak flow meters. Peak flow meters measure the highest airflow during a forced expiration.
- Daily peak flow monitoring. This is recommended for patients who meet one or more of the following criteria: have moderate or severe persistent asthma, have poor perception of changes in airflow or worsening symptoms, have unexplained response to environmental or occupational exposures, or at the discretion of the clinician or patient.
- Function. If peak flow monitoring is used, it helps measure asthma severity and, when added to symptom monitoring, indicates the current degree of asthma control.
Nursing Management
The immediate care of patients with asthma depends on the severity of the symptoms.
Assessment of a patient with asthma includes the following:
- Assess the patient’s respiratory status by monitoring the severity of the symptoms.
- Assess for breath sounds.
- Assess the patient’s peak flow.
- Assess the level of oxygen saturation through the pulse oximeter.
- Monitor the patient’s vital signs.
Based on the data gathered, the nursing diagnoses appropriate for the patient with asthma include:
- Ineffective airway clearance related to increased production of mucus and bronchospasm.
- Impaired gas exchange related to altered delivery of inspired O2.
- Anxiety related to perceived threat of death.
Main Article: 5 Bronchial Asthma Nursing Care Plans
To achieve success in the treatment of a patient with asthma, the following goals should be applied:
- Maintenance of airway patency .
- Expectoration of secretions.
- Demonstration of absence/reduction of congestion with breath sounds clear, respirations noiseless, improved oxygen exchange.
- Verbalization of understanding of causes and therapeutic management regimen.
- Demonstration of behaviors to improve or maintain clear airway.
- Identification of potential complications and how to initiate appropriate preventive or corrective actions.
The nurse generally performs the following interventions:
- Assess history. Obtain a history of allergic reactions to medications before administering medications.
- Assess respiratory status . Assess the patient’s respiratory status by monitoring the severity of symptoms, breath sounds, peak flow, pulse oximetry, and vital signs.
- Assess medications. Identify medications that the patient is currently taking. Administer medications as prescribed and monitor the patient’s responses to those medications; medications may include an antibiotic if the patient has an underlying respiratory infection .
- Pharmacologic therapy. Administer medications as prescribed and monitor patient’s responses to medications.
- Fluid therapy . Administer fluids if the patient is dehydrated.
To determine the effectiveness of the plan of care, evaluation must be performed. The following must be evaluated:
- Maintenance of airway patency.
- Expectoration or clearance of secretions.
- Absence /reduction of congestion with breath sound clear, noiseless respirations, and improved oxygen exchange.
- Verbalized understanding of causes and therapeutic management regimen.
- Demonstrated behaviors to improve or maintain clear airway.
- Identified potential complications and how to initiate appropriate preventive or corrective actions.
A major challenge is to implement basic asthma management principles at the home and community level.
- Collaboration. The complex therapy of treating asthma at home needs collaboration between the patient and the health care provider to determine the desired outcomes and to formulate a plan to achieve those outcomes.
- Health education. Patient teaching is a critical component of care for patients with asthma. Teach patient and family about asthma (chronic inflammatory), purpose and action of medications, triggers to avoid and how to do so, and proper inhalation technique. Instruct patient and family about peak-flow monitoring. Obtain current educational materials for the patient based on the patient’s diagnosis, causative factors, educational level, and cultural background.
- Compliance to therapy. Nurses should emphasize adherence to the prescribed therapy, preventive measures, and the need to keep follow-up appointments with health care providers. Teach patient how to implement an action plan and how and when to seek assistance.
- Home visits. Home visits by the nurse to assess the home environment for allergens may be indicated for patients with recurrent exacerbations.
Documentation is a necessary part of the nursing care provided, and the following data must be documented:
- Related factors for individual client.
- Breath sounds, presence and character of secretions, and use of accessory muscles for breathing.
- Character of cough and sputum.
- Respiratory rate, pulse oximetry/o2 saturation, and vital signs.
- Plan of care and who is involved in planning .
- Teaching plan.
- Client’s response to interventions, teaching, and actions performed.
- Use of respiratory devices/airway adjuncts.
- Response to medications administered.
- Attainment or progress towards desired outcomes.
- Modifications to the plan of care.
Posts related to Asthma:
- Asthma and COPD NCLEX Practice Quiz 1 (50 Items)
- Asthma and COPD NCLEX Practice Quiz 2 (50 Items)
- 5 Bronchial Asthma Nursing Care Plans
5 thoughts on “Asthma”
Perfect for students
I would like to use some of this key information in a student case study that I’m writing but am hesitant to do so because I don’t see enough information here about how to cite the reference. I suggest you add a widget/button that provides an APA style reference citation. It would also bring alot of free advertisement. : )
Thanks I really got what I wanted
You are really great, will like to meet you one day in America
Great lecture
Leave a Comment Cancel reply
Case Study: Managing Severe Asthma in an Adult
—he follows his treatment plan, but this 40-year-old male athlete has asthma that is not well-controlled. what’s the next step.
By Kirstin Bass, MD, PhD Reviewed by Michael E. Wechsler, MD, MMSc
This case presents a patient with poorly controlled asthma that remains refractory to treatment despite use of standard-of-care therapeutic options. For patients such as this, one needs to embark on an extensive work-up to confirm the diagnosis, assess for comorbidities, and finally, to consider different therapeutic options.

Case presentation and patient history
Mr. T is a 40-year-old recreational athlete with a medical history significant for asthma, for which he has been using an albuterol rescue inhaler approximately 3 times per week for the past year. During this time, he has also been waking up with asthma symptoms approximately twice a month, and has had three unscheduled asthma visits for mild flares. Based on the National Asthma Education and Prevention Program guidelines , Mr. T has asthma that is not well controlled. 1
As a result of these symptoms, spirometry was performed revealing a forced expiratory volume in the first second (FEV1) of 78% predicted. Mr. T then was prescribed treatment with a low-dose corticosteroid, fluticasone 44 mcg at two puffs twice per day. However, he remained symptomatic and continued to use his rescue inhaler 3 times per week. Therefore, he was switched to a combination inhaled steroid and long-acting beta-agonist (LABA) (fluticasone propionate 250 mcg and salmeterol 50 mcg, one puff twice a day) by his primary care doctor.
Initial pulmonary assessment Even with this step up in his medication, Mr. T continued to be symptomatic and require rescue inhaler use. Therefore, he was referred to a pulmonologist, who performed the initial work-up shown here:
- Spirometry, pre-albuterol: FEV1 79%, post-albuterol: 12% improvement
- Methacholine challenge: PC 20 : 1.0 mg/mL
- Chest X-ray: Within normal limits
Continued pulmonary assessment His dose of inhaled corticosteroid (ICS) and LABA was increased to fluticasone 500 mcg/salmeterol 50 mcg, one puff twice daily. However, he continued to have symptoms and returned to the pulmonologist for further work-up, shown here:
- Chest computed tomography (CT): Normal lung parenchyma with no scarring or bronchiectasis
- Sinus CT: Mild mucosal thickening
- Complete blood count (CBC): Within normal limits, white blood cells (WBC) 10.0 K/mcL, 3% eosinophils
- Immunoglobulin E (IgE): 25 IU/mL
- Allergy-skin test: Positive for dust, trees
- Exhaled NO: Fractional exhaled nitric oxide (FeNO) 53 parts per billion (pbb)
Assessment for comorbidities contributing to asthma symptoms After this work-up, tiotropium was added to his medication regimen. However, he remained symptomatic and had two more flares over the next 3 months. He was assessed for comorbid conditions that might be affecting his symptoms, and results showed:
- Esophagram/barium swallow: Negative
- Esophageal manometry: Negative
- Esophageal impedance: Within normal limits
- ECG: Within normal limits
- Genetic testing: Negative for cystic fibrosis, alpha1 anti-trypsin deficiency
The ear, nose, and throat specialist to whom he was referred recommended only nasal inhaled steroids for his mild sinus disease and noted that he had a normal vocal cord evaluation.
Following this extensive work-up that transpired over the course of a year, Mr. T continued to have symptoms. He returned to the pulmonologist to discuss further treatment options for his refractory asthma.
Diagnosis Mr. T has refractory asthma. Work-up for this condition should include consideration of other causes for the symptoms, including allergies, gastroesophageal reflux disease, cardiac disease, sinus disease, vocal cord dysfunction, or genetic diseases, such as cystic fibrosis or alpha1 antitrypsin deficiency, as was performed for Mr. T by his pulmonary team.
Treatment options When a patient has refractory asthma, treatment options to consider include anticholinergics (tiotropium, aclidinium), leukotriene modifiers (montelukast, zafirlukast), theophylline, anti-immunoglobulin E (IgE) antibody therapy with omalizumab, antibiotics, bronchial thermoplasty, or enrollment in a clinical trial evaluating the use of agents that modulate the cell signaling and immunologic responses seen in asthma.
Treatment outcome Mr. T underwent bronchial thermoplasty for his asthma. One year after the procedure, he reports feeling great. He has not taken systemic steroids for the past year, and his asthma remains controlled on a moderate dose of ICS and a LABA. He has also been able to resume exercising on a regular basis.
Approximately 10% to 15% of asthma patients have severe asthma refractory to the commonly available medications. 2 One key aspect of care for this patient population is a careful workup to exclude other comorbidities that could be contributing to their symptoms. Following this, there are several treatment options to consider, as in recent years there have been several advances in the development of asthma therapeutics. 2
Treatment options for refractory asthma There are a number of currently approved therapies for severe, refractory asthma. In addition to therapy with ICS or combination therapies with ICS and LABAs, leukotriene antagonists have good efficacy in asthma, especially in patients with prominent allergic or exercise symptoms. 2 The anticholinergics, such as tiotropium, which was approved for asthma in 2015, enhance bronchodilation and are useful adjuncts to ICS. 3-5 Omalizumab is a monoclonal antibody against IgE recommended for use in severe treatment-refractory allergic asthma in patients with atopy. 2 A nonmedication therapeutic option to consider is bronchial thermoplasty, a bronchoscopic procedure that uses thermal energy to disrupt bronchial smooth muscle. 6,7
Personalizing treatment for each patient It is important to personalize treatment based on individual characteristics or phenotypes that predict the patient's likely response to treatment, as well as the patient's preferences and practical issues, such as adherence and cost. 8
In this case, tiotropium had already been added to Mr. T's medications and his symptoms continued. Although addition of a leukotriene modifier was an option for him, he did not wish to add another medication to his care regimen. Omalizumab was not added partly for this reason, and also because of his low IgE level. As his bronchoscopy was negative, it was determined that a course of antibiotics would not be an effective treatment option for this patient. While vitamin D insufficiency has been associated with adverse outcomes in asthma, T's vitamin D level was tested and found to be sufficient.
We discussed the possibility of Mr. T's enrollment in a clinical trial. However, because this did not guarantee placement within a treatment arm and thus there was the possibility of receiving placebo, he opted to undergo bronchial thermoplasty.
Bronchial thermoplasty Bronchial thermoplasty is effective for many patients with severe persistent asthma, such as Mr. T. This procedure may provide additional benefits to, but does not replace, standard asthma medications. During the procedure, thermal energy is delivered to the airways via a bronchoscope to reduce excess airway smooth muscle and limit its ability to constrict the airways. It is an outpatient procedure performed over three sessions by a trained physician. 9
The effects of bronchial thermoplasty have been studied in several trials. The first large-scale multicenter randomized controlled study was the Asthma Intervention Research (AIR) Trial , which enrolled patients with moderate to severe asthma. 10 In this trial, patients who underwent the procedure had a significant improvement in asthma symptoms as measured by symptom-free days and scores on asthma control and quality of life questionnaires, as well as reductions in mild exacerbations and increases in morning peak expiratory flow. 10 Shortly after the AIR trial, the Research in Severe Asthma (RISA) trial was conducted to evaluate bronchial thermoplasty in patients with more severe, symptomatic asthma. 11 In this population, bronchial thermoplasty resulted in a transient worsening of asthma symptoms, with a higher rate of hospitalizations during the treatment period. 11 Hospitalization rate equalized between the treatment and control groups in the posttreatment period, however, and the treatment group showed significant improvements in rescue medication use, prebronchodilator forced expiratory volume in the first second (FEV1) % predicted, and asthma control questionnaire scores. 11
The AIR-2 trial followed, which was a multicenter, randomized, double-blind, sham-controlled study of 288 patients with severe asthma. 6 Similar to the RISA trial, patients in the treatment arm of this trial experienced an increase in adverse respiratory effects during the treatment period, the most common being airway irritation (including wheezing, chest discomfort, cough, and chest pain) and upper respiratory tract infections. 6
The majority of adverse effects occurred within 1 day of the procedure and resolved within 7 days. 6 In this study, bronchial thermoplasty was found to significantly improve quality of life, as well as reduce the rate of severe exacerbations by 32%. 6 Patients who underwent the procedure also reported fewer adverse respiratory effects, fewer days lost from work, school, or other activities due to asthma, and an 84% risk reduction in emergency department visits. 6
Long-term (5-year) follow-up studies have been conducted for patients in both the AIR and the AIR-2 trials. In patients who underwent bronchial thermoplasty in either study, the rate of adverse respiratory effects remained stable in years 2 to 5 following the procedure, with no increase in hospitalizations or emergency department visits. 7,12 Additionally, FEV1 remained stable throughout the 5-year follow-up period. 7,12 This finding was maintained in patients enrolled in the AIR-2 trial despite decreased use of daily ICS. 7
Bronchial thermoplasty is an important addition to the asthma treatment armamentarium. 7 This treatment is currently approved for individuals with severe persistent asthma who remain uncontrolled despite the use of an ICS and LABA. Several clinical trials with long-term follow-up have now demonstrated its safety and ability to improve quality of life in patients with severe asthma, such as Mr. T.
Severe asthma can be a challenge to manage. Patients with this condition require an extensive workup, but there are several treatments currently available to help manage these patients, and new treatments are continuing to emerge. Managing severe asthma thus requires knowledge of the options available as well as consideration of a patient's personal situation-both in terms of disease phenotype and individual preference. In this case, the patient expressed a strong desire to not add any additional medications to his asthma regimen, which explained the rationale for choosing to treat with bronchial thermoplasty. Personalized treatment necessitates exploring which of the available or emerging options is best for each individual patient.
Published: April 16, 2018
- 1. National Asthma Education and Prevention Program: Asthma Care Quick Reference.
- 2. Olin JT, Wechsler ME. Asthma: pathogenesis and novel drugs for treatment. BMJ . 2014;349:g5517.
- 3. Boehringer Ingelheim. Asthma: U.S. FDA approves new indication for SPIRIVA Respimat [press release]. September 16, 2015.
- 4. Peters SP, Kunselman SJ, Icitovic N, et al. Tiotropium bromide step-up therapy for adults with uncontrolled asthma. N Engl J Med . 2010;363:1715-1726.
- 5. Kerstjens HA, Engel M, Dahl R. Tiotropium in asthma poorly controlled with standard combination therapy. N Engl J Med . 2012;367:1198-1207.
- 6. Castro M, Rubin AS, Laviolette M, et al. Effectiveness and safety of bronchial thermoplasty in the treatment of severe asthma: a multicenter, randomized, double-blind, sham-controlled clinical trial. Am J Respir Crit Care Med . 2010;181:116-124.
- 7. Wechsler ME, Laviolette M, Rubin AS, et al. Bronchial thermoplasty: long-term safety and effectiveness in patients with severe persistent asthma. J Allergy Clin Immunol . 2013;132:1295-1302.
- 8. Global Initiative for Asthma: Pocket Guide for Asthma Management and Prevention (for Adults and Children Older than 5 Years).
- 10. Cox G, Thomson NC, Rubin AS, et al. Asthma control during the year after bronchial thermoplasty. N Engl J Med . 2007;356:1327-1337.
- 11. Pavord ID, Cox G, Thomson NC, et al. Safety and efficacy of bronchial thermoplasty in symptomatic, severe asthma. Am J Respir Crit Care Med . 2007;176:1185-1191.
- 12. Thomson NC, Rubin AS, Niven RM, et al. Long-term (5 year) safety of bronchial thermoplasty: Asthma Intervention Research (AIR) trial. BMC Pulm Med . 2011;11:8.
Treatable traits and future exacerbation risk in severe asthma, baker’s asthma, the long-term trajectory of mild asthma, age, gender, & systemic corticosteroid comorbidities, ask the expert: william busse, md, challenges the current definition of the atopic march, considering the curveballs in asthma treatment, do mucus plugs play a bigger role in chronic severe asthma than previously thought, an emerging subtype of copd is associated with early respiratory disease.

Nursing Case Study for Pediatric Asthma
Watch More! Unlock the full videos with a FREE trial
Included In This Lesson
Study tools.
Access More! View the full outline and transcript with a FREE trial
Anthony is a 6-yr-old male patient brought to the pediatric ER with a history of asthma since he came home from the NICU as an infant. He lives with his parents, Bob and Josh, who adopted him after fostering him from age 4 months. They have tried the usual nebulizer treatments but Anthony is not responding as usual, so they brought him for evaluation.
Initial assessment in triage reveals both inspiratory and expiratory wheezes, dyspnea, tachypnea, diaphoresis, and retractions.
BP 70/40 mmHg SpO2 93% on room air HR 131 bpm RR 32bpm at rest Temp 38.3°C
What physiologic issue is Anthony suffering from based on the assessment findings?
- Respiratory distress is evidenced by both vital signs and physical assessment findings. His RR and HR are high. He is also sweating and having retractions which may indicate he is working hard to try to establish oxygen exchange.
What signs and symptoms might occur that would show worsening of his condition?
- Skin color changes (i.e. blue or bluish around the mouth or even inside the mouth, blue nail beds, gray or pale compared to usual)
- Grunting on exhalation (this indicates the body is trying to keep air in the lungs)
- Stridor (this is heard in the upper airway and can be an ominous sign)
- Changes in the level of consciousness (becoming lethargic or drowsy)
Anthony is pale but not gray. His lips do indicate a very faint bluish tinge. He can speak but it appears difficult.
What medications might the nurse expect the provider to order?
- Short-acting beta-agonists (SABAs)
- Racemic albuterol – A racemic mixture of albuterol (salbutamol) is the primary SABA used for quick relief of acute asthma symptoms and exacerbations.
- Levalbuterol – Levalbuterol (Levosalbutamol), the R-enantiomer, is the active isomer of racemic albuterol that confers the bronchodilator effects. Levalbuterol is approved in the United States for the treatment of bronchospasm in children ≥4 years of age via hydrofluoroalkane (HFA) metered-dose inhaler (MDI) and ≥6 years of age via solution for nebulizer
What side effects might occur from the medications ordered?
- “The most common side effects are tremor, increased heart rate, and palpitations” Anthony may report feeling jittery due to the activation of beta receptors.
After administration of racemic albuterol, Anthony now has a RR of 22 and O2 saturation of 95% on room air. However, the provider decides to admit him to the inpatient pediatric observation unit. His parents ask if there are ways to keep him from continually being admitted to the hospital.
What are some education topics to bring up to Anthony’s parents?
- Controlling asthma triggers — The factors that set off or worsen asthma symptoms are called “triggers.” Identifying and avoiding asthma triggers is essential to keeping symptoms under control. Common asthma triggers generally fall into several categories:
- Allergens (including dust mites, pollen, mold, cockroaches, mice, cats, and dogs)
- Respiratory infections, such as the common cold or the flu
- Irritants (such as tobacco smoke, chemicals, and strong odors or fumes)
- Exercise or other physical activity
What does the nurse understand about this medication?
- Systemic corticosteroids are an essential treatment option for many disease states, especially asthma. These medications reduce the length and severity of asthma exacerbations and reduce the need for hospitalization or ED visits. It is important for asthma patients to receive prednisolone as soon as possible after the onset of symptoms that are bronchodilator-unresponsive to attain these benefits.
- Although usually prescribed for a 5- to 7-day period, oral corticosteroids are not without adverse effects. The most common adverse effects are the same for the majority of oral corticosteroids and include increased appetite, weight gain, flushed face.
- Increased risk of infections, especially with common bacterial, viral and fungal microorganisms. Thinning bones (osteoporosis) and fractures happen over time, be mindful this may cause problems in an energetic child. Suppressed adrenal gland hormone production may result in a variety of signs and symptoms, including severe fatigue, loss of appetite, nausea and muscle weakness.
Anthony sleeps during the night shift and the next day, his pediatrician makes rounds and discusses a change in the severity rating of Anthony’s asthma.
What does the nurse know about asthma severity and how it is determined?
- Asthma severity is the intrinsic intensity of the disease. Assessment of asthma severity is made on the basis of components of current impairment and future risk. The severity is determined by the most severe category measured
Bob and Josh are interested in meeting with respiratory therapy for assistance with inhalers. They say that Anthony has trouble using inhaler devices.
Inviting respiratory therapy to provide parent teaching is an example of what? How can this department help the family?
- Interdisciplinary team collaboration.
- Teaching about medications, proper inhaler (or other equipment) use, thorough explanation of peak expiratory flow (PEF) measuring, ways to help control RR.
After lunch, Anthony is ready to be discharged. His parents verbalize gratitude to the staff and thank the team for helping with education.
What can the nurse help Bob and Josh start to establish to try to help them with Anthony’s condition?
- Setting goals and planning. Preparing for an action plan (“Asthma ‘action plan’ is a form or document that your child’s provider can help you put together; it includes instructions about how to monitor symptoms and what to do when they happen. Asthma action plans are available for children up to five years old, for children five years and older and adults and for school. An action plan can tell you when to add or increase medications, when to call your child’s provider, and when to get immediate emergency help. This can help you know what to do in the event of an asthma attack. Different people can have different action plans, and your child’s action plan will likely change over time.”)
View the FULL Outline
When you start a FREE trial you gain access to the full outline as well as:
- SIMCLEX (NCLEX Simulator)
- 6,500+ Practice NCLEX Questions
- 2,000+ HD Videos
- 300+ Nursing Cheatsheets
“Would suggest to all nursing students . . . Guaranteed to ease the stress!”
References:
View the full transcript, nursing case studies.

This nursing case study course is designed to help nursing students build critical thinking. Each case study was written by experienced nurses with first hand knowledge of the “real-world” disease process. To help you increase your nursing clinical judgement (critical thinking), each unfolding nursing case study includes answers laid out by Blooms Taxonomy to help you see that you are progressing to clinical analysis.We encourage you to read the case study and really through the “critical thinking checks” as this is where the real learning occurs. If you get tripped up by a specific question, no worries, just dig into an associated lesson on the topic and reinforce your understanding. In the end, that is what nursing case studies are all about – growing in your clinical judgement.
Nursing Case Studies Introduction
Cardiac nursing case studies.
- 6 Questions
- 7 Questions
- 5 Questions
- 4 Questions
GI/GU Nursing Case Studies
- 2 Questions
- 8 Questions
Obstetrics Nursing Case Studies
Respiratory nursing case studies.
- 10 Questions
Pediatrics Nursing Case Studies
- 3 Questions
- 12 Questions
Neuro Nursing Case Studies
Mental health nursing case studies.
- 9 Questions
Metabolic/Endocrine Nursing Case Studies
Other nursing case studies.
Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- Perspective
- Open access
- Published: 16 October 2014
A woman with asthma: a whole systems approach to supporting self-management
- Hilary Pinnock 1 ,
- Elisabeth Ehrlich 1 ,
- Gaylor Hoskins 2 &
- Ron Tomlins 3
npj Primary Care Respiratory Medicine volume 24 , Article number: 14063 ( 2014 ) Cite this article
16k Accesses
2 Citations
6 Altmetric
Metrics details
- Health care
A 35-year-old lady attends for review of her asthma following an acute exacerbation. There is an extensive evidence base for supported self-management for people living with asthma, and international and national guidelines emphasise the importance of providing a written asthma action plan. Effective implementation of this recommendation for the lady in this case study is considered from the perspective of a patient, healthcare professional, and the organisation. The patient emphasises the importance of developing a partnership based on honesty and trust, the need for adherence to monitoring and regular treatment, and involvement of family support. The professional considers the provision of asthma self-management in the context of a structured review, with a focus on a self-management discussion which elicits the patient’s goals and preferences. The organisation has a crucial role in promoting, enabling and providing resources to support professionals to provide self-management. The patient’s asthma control was assessed and management optimised in two structured reviews. Her goal was to avoid disruption to her work and her personalised action plan focused on achieving that goal.
Similar content being viewed by others

Barriers to implementing asthma self-management in Malaysian primary care: qualitative study exploring the perspectives of healthcare professionals

The self-management abilities test (SMAT): a tool to identify the self-management abilities of adults with bronchiectasis

Improving primary care management of asthma: do we know what really works?
A 35-year-old sales representative attends the practice for an asthma review. Her medical record notes that she has had asthma since childhood, and although for many months of the year her asthma is well controlled (when she often reduces or stops her inhaled steroids), she experiences one or two exacerbations a year requiring oral steroids. These are usually triggered by a viral upper respiratory infection, though last summer when the pollen count was particularly high she became tight chested and wheezy for a couple of weeks.
Her regular prescription is for fluticasone 100 mcg twice a day, and salbutamol as required. She has a young family and a busy lifestyle so does not often manage to find time to attend the asthma clinic. A few weeks previously, an asthma attack had interfered with some important work-related travel, and she has attended the clinic on this occasion to ask about how this can be managed better in the future. There is no record of her having been given an asthma action plan.
What do we know about asthma self-management? The academic perspective
Supported self-management reduces asthma morbidity.
The lady in this case study is struggling to maintain control of her asthma within the context of her busy professional and domestic life. The recent unfortunate experience which triggered this consultation offers a rare opportunity to engage with her and discuss how she can manage her asthma better. It behoves the clinician whom she is seeing (regardless of whether this is in a dedicated asthma clinic or an appointment in a routine general practice surgery) to grasp the opportunity and discuss self-management and provide her with a (written) personalised asthma action plan (PAAP).
The healthcare professional advising the lady is likely to be aware that international and national guidelines emphasise the importance of supporting self-management. 1 – 4 There is an extensive evidence base for asthma self-management: a recent synthesis identified 22 systematic reviews summarising data from 260 randomised controlled trials encompassing a broad range of demographic, clinical and healthcare contexts, which concluded that asthma self-management reduces emergency use of healthcare resources, including emergency department visits, hospital admissions and unscheduled consultations and improves markers of asthma control, including reduced symptoms and days off work, and improves quality of life. 1 , 2 , 5 – 12 Health economic analysis suggests that it is not only clinically effective, but also a cost-effective intervention. 13
Personalised asthma action plans
Key features of effective self-management approaches are:
Self-management education should be reinforced by provision of a (written) PAAP which reminds patients of their regular treatment, how to monitor and recognise that control is deteriorating and the action they should take. 14 – 16 As an adult, our patient can choose whether she wishes to monitor her control with symptoms or by recording peak flows (or a combination of both). 6 , 8 , 9 , 14 Symptom-based monitoring is generally better in children. 15 , 16
Plans should have between two and three action points including emergency doses of reliever medication; increasing low dose (or recommencing) inhaled steroids; or starting a course of oral steroids according to severity of the exacerbation. 14
Personalisation of the action plan is crucial. Focussing specifically on what actions she could take to prevent a repetition of the recent attack is likely to engage her interest. Not all patients will wish to start oral steroids without advice from a healthcare professional, though with her busy lifestyle and travel our patient is likely to be keen to have an emergency supply of prednisolone. Mobile technology has the potential to support self-management, 17 , 18 though a recent systematic review concluded that none of the currently available smart phone ‘apps’ were fit for purpose. 19
Identification and avoidance of her triggers is important. As pollen seems to be a trigger, management of allergic rhinitis needs to be discussed (and included in her action plan): she may benefit from regular use of a nasal steroid spray during the season. 20
Self-management as recommended by guidelines, 1 , 2 focuses narrowly on adherence to medication/monitoring and the early recognition/remediation of exacerbations, summarised in (written) PAAPs. Patients, however, may want to discuss how to reduce the impact of asthma on their life more generally, 21 including non-pharmacological approaches.
Supported self-management
The impact is greater if self-management education is delivered within a comprehensive programme of accessible, proactive asthma care, 22 and needs to be supported by ongoing regular review. 6 With her busy lifestyle, our patient may be reluctant to attend follow-up appointments, and once her asthma is controlled it may be possible to make convenient arrangements for professional review perhaps by telephone, 23 , 24 or e-mail. Flexible access to professional advice (e.g., utilising diverse modes of consultation) is an important component of supporting self-management. 25
The challenge of implementation
Implementation of self-management, however, remains poor in routine clinical practice. A recent Asthma UK web-survey estimated that only 24% of people with asthma in the UK currently have a PAAP, 26 with similar figures from Sweden 27 and Australia. 28 The general practitioner may feel that they do not have time to discuss self-management in a routine surgery appointment, or may not have a supply of paper-based PAAPs readily available. 29 However, as our patient rarely finds time to attend the practice, inviting her to make an appointment for a future clinic is likely to be unsuccessful and the opportunity to provide the help she needs will be missed.
The solution will need a whole systems approach
A systematic meta-review of implementing supported self-management in long-term conditions (including asthma) concluded that effective implementation was multifaceted and multidisciplinary; engaging patients, training and motivating professionals within the context of an organisation which actively supported self-management. 5 This whole systems approach considers that although patient education, professional training and organisational support are all essential components of successful support, they are rarely effective in isolation. 30 A systematic review of interventions that promote provision/use of PAAPs highlighted the importance of organisational systems (e.g., sending blank PAAPs with recall reminders). 31 A patient offers her perspective ( Box 1 ), a healthcare professional considers the clinical challenge, and the challenges are discussed from an organisational perspective.
Box 1: What self-management help should this lady expect from her general practitioner or asthma nurse? The patient’s perspective
The first priority is that the patient is reassured that her condition can be managed successfully both in the short and the long term. A good working relationship with the health professional is essential to achieve this outcome. Developing trust between patient and healthcare professional is more likely to lead to the patient following the PAAP on a long-term basis.
A review of all medication and possible alternative treatments should be discussed. The patient needs to understand why any changes are being made and when she can expect to see improvements in her condition. Be honest, as sometimes it will be necessary to adjust dosages before benefits are experienced. Be positive. ‘There are a number of things we can do to try to reduce the impact of asthma on your daily life’. ‘Preventer treatment can protect against the effect of pollen in the hay fever season’. If possible, the same healthcare professional should see the patient at all follow-up appointments as this builds trust and a feeling of working together to achieve the aim of better self-management.
Is the healthcare professional sure that the patient knows how to take her medication and that it is taken at the same time each day? The patient needs to understand the benefit of such a routine. Medication taken regularly at the same time each day is part of any self-management regime. If the patient is unused to taking medication at the same time each day then keeping a record on paper or with an electronic device could help. Possibly the patient could be encouraged to set up a system of reminders by text or smartphone.
Some people find having a peak flow meter useful. Knowing one's usual reading means that any fall can act as an early warning to put the PAAP into action. Patients need to be proactive here and take responsibility.
Ongoing support is essential for this patient to ensure that she takes her medication appropriately. Someone needs to be available to answer questions and provide encouragement. This could be a doctor or a nurse or a pharmacist. Again, this is an example of the partnership needed to achieve good asthma control.
It would also be useful at a future appointment to discuss the patient’s lifestyle and work with her to reduce her stress. Feeling better would allow her to take simple steps such as taking exercise. It would also be helpful if all members of her family understood how to help her. Even young children can do this.
From personal experience some people know how beneficial it is to feel they are in a partnership with their local practice and pharmacy. Being proactive produces dividends in asthma control.
What are the clinical challenges for the healthcare professional in providing self-management support?
Due to the variable nature of asthma, a long-standing history may mean that the frequency and severity of symptoms, as well as what triggers them, may have changed over time. 32 Exacerbations requiring oral steroids, interrupting periods of ‘stability’, indicate the need for re-assessment of the patient’s clinical as well as educational needs. The patient’s perception of stability may be at odds with the clinical definition 1 , 33 —a check on the number of short-acting bronchodilator inhalers the patient has used over a specific period of time is a good indication of control. 34 Assessment of asthma control should be carried out using objective tools such as the Asthma Control Test or the Royal College of Physicians three questions. 35 , 36 However, it is important to remember that these assessment tools are not an end in themselves but should be a springboard for further discussion on the nature and pattern of symptoms. Balancing work with family can often make it difficult to find the time to attend a review of asthma particularly when the patient feels well. The practice should consider utilising other means of communication to maintain contact with patients, encouraging them to come in when a problem is highlighted. 37 , 38 Asthma guidelines advocate a structured approach to ensure the patient is reviewed regularly and recommend a detailed assessment to enable development of an appropriate patient-centred (self)management strategy. 1 – 4
Although self-management plans have been shown to be successful for reducing the impact of asthma, 21 , 39 the complexity of managing such a fluctuating disease on a day-to-day basis is challenging. During an asthma review, there is an opportunity to work with the patient to try to identify what triggers their symptoms and any actions that may help improve or maintain control. 38 An integral part of personalised self-management education is the written PAAP, which gives the patient the knowledge to respond to the changes in symptoms and ensures they maintain control of their asthma within predetermined parameters. 9 , 40 The PAAP should include details on how to monitor asthma, recognise symptoms, how to alter medication and what to do if the symptoms do not improve. The plan should include details on the treatment to be taken when asthma is well controlled, and how to adjust it when the symptoms are mild, moderate or severe. These action plans need to be developed between the doctor, nurse or asthma educator and the patient during the review and should be frequently reviewed and updated in partnership (see Box 1). Patient preference as well as clinical features such as whether she under- or over-perceives her symptoms should be taken into account when deciding whether the action plan is peak flow or symptom-driven. Our patient has a lot to gain from having an action plan. She has poorly controlled asthma and her lifestyle means that she will probably see different doctors (depending who is available) when she needs help. Being empowered to self-manage could make a big difference to her asthma control and the impact it has on her life.
The practice should have protocols in place, underpinned by specific training to support asthma self-management. As well as ensuring that healthcare professionals have appropriate skills, this should include training for reception staff so that they know what action to take if a patient telephones to say they are having an asthma attack.
However, focusing solely on symptom management strategies (actions) to follow in the presence of deteriorating symptoms fails to incorporate the patients’ wider views of asthma, its management within the context of her/his life, and their personal asthma management strategies. 41 This may result in a failure to use plans to maximise their health potential. 21 , 42 A self-management strategy leading to improved outcomes requires a high level of patient self-efficacy, 43 a meaningful partnership between the patient and the supporting health professional, 42 , 44 and a focused self-management discussion. 14
Central to both the effectiveness and personalisation of action plans, 43 , 45 in particular the likelihood that the plan will lead to changes in patients’ day-to-day self-management behaviours, 45 is the identification of goals. Goals are more likely to be achieved when they are specific, important to patients, collaboratively set and there is a belief that these can be achieved. Success depends on motivation 44 , 46 to engage in a specific behaviour to achieve a valued outcome (goal) and the ability to translate the behavioural intention into action. 47 Action and coping planning increases the likelihood that patient behaviour will actually change. 44 , 46 , 47 Our patient has a goal: she wants to avoid having her work disrupted by her asthma. Her personalised action plan needs to explicitly focus on achieving that goal.
As providers of self-management support, health professionals must work with patients to identify goals (valued outcomes) that are important to patients, that may be achievable and with which they can engage. The identification of specific, personalised goals and associated feasible behaviours is a prerequisite for the creation of asthma self-management plans. Divergent perceptions of asthma and how to manage it, and a mismatch between what patients want/need from these plans and what is provided by professionals are barriers to success. 41 , 42
What are the challenges for the healthcare organisation in providing self-management support?
A number of studies have demonstrated the challenges for primary care physicians in providing ongoing support for people with asthma. 31 , 48 , 49 In some countries, nurses and other allied health professionals have been trained as asthma educators and monitor people with stable asthma. These resources are not always available. In addition, some primary care services are delivered in constrained systems where only a few minutes are available to the practitioner in a consultation, or where only a limited range of asthma medicines are available or affordable. 50
There is recognition that the delivery of quality care depends on the competence of the doctor (and supporting health professionals), the relationship between the care providers and care recipients, and the quality of the environment in which care is delivered. 51 This includes societal expectations, health literacy and financial drivers.
In 2001, the Australian Government adopted a programme developed by the General Practitioner Asthma Group of the National Asthma Council Australia that provided a structured approach to the implementation of asthma management guidelines in a primary care setting. 52 Patients with moderate-to-severe asthma were eligible to participate. The 3+ visit plan required confirmation of asthma diagnosis, spirometry if appropriate, assessment of trigger factors, consideration of medication and patient self-management education including provision of a written PAAP. These elements, including regular medical review, were delivered over three visits. Evaluation demonstrated that the programme was beneficial but that it was difficult to complete the third visit in the programme. 53 – 55 Accordingly, the programme, renamed the Asthma Cycle of Care, was modified to incorporate two visits. 56 Financial incentives are provided to practices for each patient who receives this service each year.
Concurrently, other programmes were implemented which support practice-based care. Since 2002, the National Asthma Council has provided best-practice asthma and respiratory management education to health professionals, 57 and this programme will be continuing to 2017. The general practitioner and allied health professional trainers travel the country to provide asthma and COPD updates to groups of doctors, nurses and community pharmacists. A number of online modules are also provided. The PACE (Physician Asthma Care Education) programme developed by Noreen Clark has also been adapted to the Australian healthcare system. 58 In addition, a pharmacy-based intervention has been trialled and implemented. 59
To support these programmes, the National Asthma Council ( www.nationalasthma.org.au ) has developed resources for use in practices. A strong emphasis has been on the availability of a range of PAAPs (including plans for using adjustable maintenance dosing with ICS/LABA combination inhalers), plans for indigenous Australians, paediatric plans and plans translated into nine languages. PAAPs embedded in practice computer systems are readily available in consultations, and there are easily accessible online paediatric PAAPs ( http://digitalmedia.sahealth.sa.gov.au/public/asthma/ ). A software package, developed in the UK, can be downloaded and used to generate a pictorial PAAP within the consultation. 60
One of the strongest drivers towards the provision of written asthma action plans in Australia has been the Asthma Friendly Schools programme. 61 , 62 Established with Australian Government funding and the co-operation of Education Departments of each state, the Asthma Friendly Schools programme engages schools to address and satisfy a set of criteria that establishes an asthma-friendly environment. As part of accreditation, the school requires that each child with asthma should have a written PAAP prepared by their doctor to assist (trained) staff in managing a child with asthma at school.
The case study continues...
The initial presentation some weeks ago was during an exacerbation of asthma, which may not be the best time to educate a patient. It is, however, a splendid time to build on their motivation to feel better. She agreed to return after her asthma had settled to look more closely at her asthma control, and an appointment was made for a routine review.
At this follow-up consultation, the patient’s diagnosis was reviewed and confirmed and her trigger factors discussed. For this lady, respiratory tract infections are the usual trigger but allergic factors during times of high pollen count may also be relevant. Assessment of her nasal airway suggested that she would benefit from better control of allergic rhinitis. Other factors were discussed, as many patients are unaware that changes in air temperature, exercise and pets can also trigger asthma exacerbations. In addition, use of the Asthma Control Test was useful as an objective assessment of control as well as helping her realise what her life could be like! Many people with long-term asthma live their life within the constraints of their illness, accepting that is all that they can do.
After assessing the level of asthma control, a discussion about management options—trigger avoidance, exercise and medicines—led to the development of a written PAAP. Asthma can affect the whole family, and ways were explored that could help her family understand why it is important that she finds time in the busy domestic schedules to take her regular medication. Family and friends can also help by understanding what triggers her asthma so that they can avoid exposing her to perfumes, pollens or pets that risk triggering her symptoms. Information from the national patient organisation was provided to reinforce the messages.
The patient agreed to return in a couple of weeks, and a recall reminder was set up. At the second consultation, the level of control since the last visit will be explored including repeat spirometry, if appropriate. Further education about the pathophysiology of asthma and how to recognise early warning signs of loss of control can be given. Device use will be reassessed and the PAAP reviewed. Our patient’s goal is to avoid disruption to her work and her PAAP will focus on achieving that goal. Finally, agreement will be reached with the patient about future routine reviews, which, now that she has a written PAAP, could be scheduled by telephone if all is well, or face-to-face if a change in her clinical condition necessitates a more comprehensive review.
Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention, 2012. Available from: http://www.ginasthma.org (accessed July 2013).
British Thoracic Society/Scottish Intercollegiate Guideline Network British Guideline on the Management of Asthma. Thorax 2008; 63 (Suppl 4 iv1–121, updated version available from: http://www.sign.ac.uk (accessed January 2014).
Article Google Scholar
National Asthma Council Australia. Australian Asthma Handbook. Available from: http://www.nationalasthma.org.au/handbook (accessed May 2014).
National Asthma Education and Prevention Program (NAEPP) Coordinating Committee. Expert Panel Report 3 (EPR3): Guidelines for the Diagnosis and Management of Asthma. Available from: https://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.htm (accessed May 2014).
Taylor SJC, Pinnock H, Epiphaniou E, Pearce G, Parke H . A rapid synthesis of the evidence on interventions supporting self-management for people with long-term conditions. (PRISMS Practical Systematic Review of Self-Management Support for long-term conditions). Health Serv Deliv Res (in press).
Gibson PG, Powell H, Wilson A, Abramson MJ, Haywood P, Bauman A et al. Self-management education and regular practitioner review for adults with asthma. Cochrane Database Syst Rev 2002: (Issue 3) Art No. CD001117.
Tapp S, Lasserson TJ, Rowe BH . Education interventions for adults who attend the emergency room for acute asthma. Cochrane Database Syst Rev 2007: (Issue 3) Art No. CD003000.
Powell H, Gibson PG . Options for self-management education for adults with asthma. Cochrane Database Syst Rev 2002: (Issue 3) Art No: CD004107.
Toelle B, Ram FSF . Written individualised management plans for asthma in children and adults. Cochrane Database Syst Rev 2004: (Issue 1) Art No. CD002171.
Lefevre F, Piper M, Weiss K, Mark D, Clark N, Aronson N . Do written action plans improve patient outcomes in asthma? An evidence-based analysis. J Fam Pract 2002; 51 : 842–848.
PubMed Google Scholar
Boyd M, Lasserson TJ, McKean MC, Gibson PG, Ducharme FM, Haby M . Interventions for educating children who are at risk of asthma-related emergency department attendance. Cochrane Database Syst Rev 2009: (Issue 2) Art No.CD001290.
Bravata DM, Gienger AL, Holty JE, Sundaram V, Khazeni N, Wise PH et al. Quality improvement strategies for children with asthma: a systematic review. Arch Pediatr Adolesc Med 2009; 163 : 572–581.
Bower P, Murray E, Kennedy A, Newman S, Richardson G, Rogers A . Self-management support interventions to reduce health care utilisation without compromising outcomes: a rapid synthesis of the evidence. Available from: http://www.nets.nihr.ac.uk/projects/hsdr/11101406 (accessed April 2014).
Gibson PG, Powell H . Written action plans for asthma: an evidence-based review of the key components. Thorax 2004; 59 : 94–99.
Article CAS Google Scholar
Bhogal SK, Zemek RL, Ducharme F . Written action plans for asthma in children. Cochrane Database Syst Rev 2006: (Issue 3) Art No. CD005306.
Zemek RL, Bhogal SK, Ducharme FM . Systematic review of randomized controlled trials examining written action plans in children: what is the plan?. Arch Pediatr Adolesc Med 2008; 162 : 157–163.
Pinnock H, Slack R, Pagliari C, Price D, Sheikh A . Understanding the potential role of mobile phone based monitoring on asthma self-management: qualitative study. Clin Exp Allergy 2007; 37 : 794–802.
de Jongh T, Gurol-Urganci I, Vodopivec-Jamsek V, Car J, Atun R . Mobile phone messaging for facilitating self-management of long-term illnesses. Cochrane Database Syst Rev 2012: (Issue 12) Art No. CD007459.
Huckvale K, Car M, Morrison C, Car J . Apps for asthma self-management: a systematic assessment of content and tools. BMC Med 2012; 10 : 144.
Allergic Rhinitis and its Impact on Asthma. Management of Allergic Rhinitis and its Impact on Asthma: Pocket Guide. ARIA 2008. Available from: http://www.whiar.org (accessed May 2014).
Ring N, Jepson R, Hoskins G, Wilson C, Pinnock H, Sheikh A et al. Understanding what helps or hinders asthma action plan use: a systematic review and synthesis of the qualitative literature. Patient Educ Couns 2011; 85 : e131–e143.
Moullec G, Gour-Provencal G, Bacon SL, Campbell TS, Lavoie KL . Efficacy of interventions to improve adherence to inhaled corticosteroids in adult asthmatics: Impact of using components of the chronic care model. Respir Med 2012; 106 : 1211–1225.
Pinnock H, Bawden R, Proctor S, Wolfe S, Scullion J, Price D et al. Accessibility, acceptability and effectiveness of telephone reviews for asthma in primary care: randomised controlled trial. BMJ 2003; 326 : 477–479.
Pinnock H, Adlem L, Gaskin S, Harris J, Snellgrove C, Sheikh A . Accessibility, clinical effectiveness and practice costs of providing a telephone option for routine asthma reviews: phase IV controlled implementation study. Br J Gen Pract 2007; 57 : 714–722.
PubMed PubMed Central Google Scholar
Kielmann T, Huby G, Powell A, Sheikh A, Price D, Williams S et al. From support to boundary: a qualitative study of the border between self care and professional care. Patient Educ Couns 2010; 79 : 55–61.
Asthma UK . Compare your care report. Asthma UK, 2013. Available from: http://www.asthma.org.uk (accessed January 2014).
Stallberg B, Lisspers K, Hasselgren M, Janson C, Johansson G, Svardsudd K . Asthma control in primary care in Sweden: a comparison between 2001 and 2005. Prim Care Respir J 2009; 18 : 279–286.
Reddel H, Peters M, Everett P, Flood P, Sawyer S . Ownership of written asthma action plans in a large Australian survey. Eur Respir J 2013; 42 . Abstract 2011.
Wiener-Ogilvie S, Pinnock H, Huby G, Sheikh A, Partridge MR, Gillies J . Do practices comply with key recommendations of the British Asthma Guideline? If not, why not? Prim Care Respir J 2007; 16 : 369–377.
Kennedy A, Rogers A, Bower P . Support for self care for patients with chronic disease. BMJ 2007; 335 : 968–970.
Ring N, Malcolm C, Wyke S, Macgillivray S, Dixon D, Hoskins G et al. Promoting the Use of Personal Asthma Action Plans: A Systematic Review. Prim Care Respir J 2007; 16 : 271–283.
Taylor DR, Bateman ED, Boulet LP, Boushey HA, Busse WW, Casale TB et al. A new perspective on concepts of asthma severity and control. Eur Respir J 2008; 32 : 545–554.
Horne R . Compliance, adherence, and concordance: implications for asthma treatment. Chest 2006; 130 (suppl): 65S–72S.
Reddel HK, Taylor DR, Bateman ED, Boulet L-P, Boushey HA, Busse WW et al. An official American Thoracic Society/European Respiratory Society statement: asthma control and exacerbations standardizing endpoints for clinical asthma trials and clinical practice. Am J Respir Crit Care Med 2009; 180 : 59–99.
Thomas M, Kay S, Pike J, Rosenzweig JR, Hillyer EV, Price D . The Asthma Control Test (ACT) as a predictor of GINA guideline-defined asthma control: analysis of a multinational cross-sectional survey. Prim Care Respir J 2009; 18 : 41–49.
Hoskins G, Williams B, Jackson C, Norman P, Donnan P . Assessing asthma control in UK primary care: use of routinely collected prospective observational consultation data to determine appropriateness of a variety of control assessment models. BMC Fam Pract 2011; 12 : 105.
Pinnock H, Fletcher M, Holmes S, Keeley D, Leyshon J, Price D et al. Setting the standard for routine asthma consultations: a discussion of the aims, process and outcomes of reviewing people with asthma in primary care. Prim Care Respir J 2010; 19 : 75–83.
McKinstry B, Hammersley V, Burton C, Pinnock H, Elton RA, Dowell J et al. The quality, safety and content of telephone and face-to-face consultations: a comparative study. Qual Saf Health Care 2010; 19 : 298–303.
Gordon C, Galloway T . Review of Findings on Chronic Disease Self-Management Program (CDSMP) Outcomes: Physical, Emotional & Health-Related Quality of Life, Healthcare Utilization and Costs . Centers for Disease Control and Prevention and National Council on Aging: Atlanta, GA, USA, 2008.
Beasley R, Crane J . Reducing asthma mortality with the self-management plan system of care. Am J Respir Crit Care Med 2001; 163 : 3–4.
Ring N, Jepson R, Pinnock H, Wilson C, Hoskins G, Sheikh A et al. Encouraging the promotion and use of asthma action plans: a cross study synthesis of qualitative and quantitative evidence. Trials 2012; 13 : 21.
Jones A, Pill R, Adams S . Qualitative study of views of health professionals and patients on guided self-management plans for asthma. BMJ 2000; 321 : 1507–1510.
Bandura A . Self-efficacy: toward a unifying theory of behavioural change. Psychol Rev 1977; 84 : 191–215.
Gollwitzer PM, Sheeran P . Implementation intentions and goal achievement: a meta-analysis of effects and processes. Adv Exp Soc Psychol 2006; 38 : 69–119.
Google Scholar
Hardeman W, Johnston M, Johnston DW, Bonetti D, Wareham NJ, Kinmonth AL . Application of the theory of planned behaviour change interventions: a systematic review. Psychol Health 2002; 17 : 123–158.
Schwarzer R . Modeling health behavior change: how to predict and modify the adoption and maintenance of health behaviors. Appl Psychol 2008; 57 : 1–29.
Sniehotta F . Towards a theory of intentional behaviour change: plans, planning, and self-regulation. Br J Health Psychol 2009; 14 : 261–273.
Okelo SO, Butz AM, Sharma R, Diette GB, Pitts SI, King TM et al. Interventions to modify health care provider adherence to asthma guidelines: a systematic review. Pediatrics 2013; 132 : 517–534.
Grol R, Grimshaw RJ . From best evidence to best practice: effective implementation of change in patients care. Lancet 2003; 362 : 1225–1230.
Jusef L, Hsieh C-T, Abad L, Chaiyote W, Chin WS, Choi Y-J et al. Primary care challenges in treating paediatric asthma in the Asia-Pacific region. Prim Care Respir J 2013; 22 : 360–362.
Donabedian A . Evaluating the quality of medical care. Milbank Q 2005; 83 : 691–729.
Fardy HJ . Moving towards organized care of chronic disease. The 3+ visit plan. Aust Fam Physician 2001; 30 : 121–125.
CAS PubMed Google Scholar
Glasgow NJ, Ponsonby AL, Yates R, Beilby J, Dugdale P . Proactive asthma care in childhood: general practice based randomised controlled trial. BMJ 2003; 327 : 659.
Douglass JA, Goemann DP, Abramson MJ . Asthma 3+ visit plan: a qualitative evaluation. Intern Med J 2005; 35 : 457–462.
Beilby J, Holton C . Chronic disease management in Australia; evidence and policy mismatch, with asthma as an example. Chronic Illn 2005; 1 : 73–80.
The Department of Health. Asthma Cycle of Care. Accessed on 14 May 2014 at http://www.health.gov.au/internet/main/publishing.nsf/Content/asthma-cycle .
National Asthma Council Australia. Asthma and Respiratory Education Program. Accessed on 14 May 2014 at http://www.nationalasthma.org.au/health-professionals/education-training/asthma-respiratory-education-program .
Patel MR, Shah S, Cabana MD, Sawyer SM, Toelle B, Mellis C et al. Translation of an evidence-based asthma intervention: Physician Asthma Care Education (PACE) in the United States and Australia. Prim Care Respir J 2013; 22 : 29–34.
Armour C, Bosnic-Anticevich S, Brilliant M, Burton D, Emmerton L, Krass I et al. Pharmacy Asthma Care Program (PACP) improves outcomes for patients in the community. Thorax 2007; 62 : 496–502.
Roberts NJ, Mohamed Z, Wong PS, Johnson M, Loh LC, Partridge MR . The development and comprehensibility of a pictorial asthma action plan. Patient Educ Couns 2009; 74 : 12–18.
Henry RL, Gibson PG, Vimpani GV, Francis JL, Hazell J . Randomised controlled trial of a teacher-led asthma education program. Pediatr Pulmonol 2004; 38 : 434–442.
National Asthma Council Australia. Asthma Friendly Schools program. Accessed on 14 May 2014 at http://www.asthmaaustralia.org.au/Asthma-Friendly-Schools.aspx .
Download references
Author information
Authors and affiliations.
Asthma UK Centre for Applied Research, Centre for Population Health Sciences, The University of Edinburgh, Edinburgh, UK,
Hilary Pinnock & Elisabeth Ehrlich
NMAHP-RU, University of Stirling, Stirling, UK,
Gaylor Hoskins
Discipline of General Practice, University of Sydney, Sydney, NSW, Australia
Ron Tomlins
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Hilary Pinnock .
Ethics declarations
Competing interests.
The authors declare no conflict of interest.
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License. The images or other third party material in this article are included in the article's Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/4.0/
Reprints and permissions
About this article
Cite this article.
Pinnock, H., Ehrlich, E., Hoskins, G. et al. A woman with asthma: a whole systems approach to supporting self-management. npj Prim Care Resp Med 24 , 14063 (2014). https://doi.org/10.1038/npjpcrm.2014.63
Download citation
Received : 23 June 2014
Revised : 15 July 2014
Accepted : 15 July 2014
Published : 16 October 2014
DOI : https://doi.org/10.1038/npjpcrm.2014.63
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies
Sign up for the Nature Briefing newsletter — what matters in science, free to your inbox daily.

- Case report
- Open access
- Published: 21 February 2018
Pediatric severe asthma: a case series report and perspectives on anti-IgE treatment
- Virginia Mirra 1 ,
- Silvia Montella 1 &
- Francesca Santamaria 1
BMC Pediatrics volume 18 , Article number: 73 ( 2018 ) Cite this article
11k Accesses
14 Citations
12 Altmetric
Metrics details
The primary goal of asthma management is to achieve disease control for reducing the risk of future exacerbations and progressive loss of lung function. Asthma not responding to treatment may result in significant morbidity. In many children with uncontrolled symptoms, the diagnosis of asthma may be wrong or adherence to treatment may be poor. It is then crucial to distinguish these cases from the truly “severe therapy-resistant” asthmatics by a proper filtering process. Herein we report on four cases diagnosed as difficult asthma, detail the workup that resulted in the ultimate diagnosis, and provide the process that led to the prescription of omalizumab.
Case presentation
All children had been initially referred because of asthma not responding to long-term treatment with high-dose inhaled steroids, long-acting β 2 -agonists and leukotriene receptor antagonists. Definitive diagnosis was severe asthma. Three out four patients were treated with omalizumab, which improved asthma control and patients’ quality of life. We reviewed the current literature on the diagnostic approach to the disease and on the comorbidities associated with difficult asthma and presented the perspectives on omalizumab treatment in children and adolescents. Based on the evidence from the literature review, we also proposed an algorithm for the diagnosis of pediatric difficult-to-treat and severe asthma.
Conclusions
The management of asthma is becoming much more patient-specific, as more and more is learned about the biology behind the development and progression of asthma. The addition of omalizumab, the first targeted biological treatment approved for asthma, has led to renewed optimism in the management of children and adolescents with atopic severe asthma.
Peer Review reports
Children with poor asthma control have an increased risk of severe exacerbations and progressive loss of lung function, which results in the relevant use of health resources and impaired quality of life (QoL) [ 1 ]. Therefore, the primary goal of asthma management at all ages is to achieve disease control [ 2 , 3 , 4 ].
According to recent international guidelines, patients with uncontrolled asthma require a prolonged maintenance treatment with high-dose inhaled corticosteroids (ICS) in association with a long-acting β 2 -agonist (LABA) plus oral leukotriene receptor antagonist (LTRA) (Table 1 ) [ 5 ].
Nevertheless, in the presence of persistent lack of control, reversible factors such as adherence to treatment or inhalation technique should be first checked for, and diseases that can masquerade as asthma should be promptly excluded. Finally, additional strategies, in particular anti-immunoglobulin E (anti-IgE) treatment (omalizumab), are suggested for patients with moderate or severe allergic asthma that remains uncontrolled in Step 4 [ 5 ].
Herein, we reviewed the demographics, clinical presentation and treatment of four patients with uncontrolled severe asthma from our institution in order to explain why we decided to prescribe omalizumab. We also provided a review of the current literature that focuses on recent advances in the diagnosis of pediatric difficult asthma and the associated comorbidities, and summarizes the perspectives on anti-IgE treatment in children and adolescents.
Case presentations
Table 2 summarizes the clinical characteristics and the triggers/comorbidities of the cases at referral to our Institution. Unfortunately, data on psychological factors, sleep apnea, and hyperventilation syndrome were not available in any case. Clinical, lung function and airway inflammation findings at baseline and after 12 months of follow-up are reported in Table 3 . In the description of our cases, we used the terminology recommended by the ERS/ATS guidelines on severe asthma [ 6 ].
A full-term male had severe preschool wheezing and, since age 3, recurrent, severe asthma exacerbations with frequent hospital admissions. At age 11, severe asthma was diagnosed. Sensitization to multiple inhalant allergens (i.e., house dust mites, dog dander, Graminaceae pollen mix, and Parietaria judaica ) and high serum IgE levels (1548 KU/l) were found. Body mass index (BMI) was within normal range. Combined treatment with increasing doses of ICS (fluticasone, up to 1000 μg/day) in association with LABA (salmeterol, 100 μg/day) plus LTRA (montelukast, 5 mg/day) has been administered over 2 years. Nevertheless, persistent symptoms and monthly hospital admissions due to asthma exacerbations despite correct inhaler technique and good adherence were reported. Parents refused to perform any test to exclude gastroesophageal reflux (GER) as comorbidity [ 6 ]. However, an ex-juvantibus 2-month-course with omeprazole was added to asthma treatment [ 7 ], but poor control persisted. Anterior rhinoscopy revealed rhinosinusitis that was treated with nasal steroids for six months [ 8 ], but asthma symptoms were unmodified. Treatment with omalizumab was added at age 12. Reduced hospital admissions for asthma exacerbations, no further need for systemic steroids, and improved QoL score (from 2.0 up to 6.7 out of a maximum of 7 points) were documented over the following months. Unfortunately, after one year of treatment, adherence to omalizumab decreased because of family complaints, and eventually parents withdrew their informed consent and discontinued omalizumab. Currently, by age 17, treatment includes inhaled salmeterol/fluticasone (100 μg/500 μg∙day -1 , respectively) plus oral montelukast (10 mg/day). Satisfactory symptom control is reported, with no asthma exacerbations.
A full-term male, who had a recurrent severe preschool wheezing, at 6 years of age developed exercise-induced asthma. At age 10, severe asthma was diagnosed. High serum IgE levels (1300 KU/l) and skin prick tests positive to house dust mites were found. Despite a 3-year treatment with progressively increasing doses of inhaled fluticasone (up to 1000 μg/day) combined with salmeterol (100 μg/day) and oral montelukast (5 mg/day), monthly hospital admissions with systemic steroids use were reported. At age 13, a 24-h esophageal impedance/pH study demonstrated the presence of acid and non-acid GER [ 7 ]. Esomeprazole was added to asthma medications, but with an incomplete clinical benefit for respiratory symptoms. Esomeprazole was withdrawn after 3 months, and parents refused to re-test for GER. As respiratory symptoms persisted uncontrolled despite treatment, severe asthma was definitively diagnosed [ 6 ]. BMI was within the normal range and anterior rhinoscopy excluded rhinosinusitis. Inhaler technique and adherence were good; thus we considered the anti-IgE treatment option [ 9 ]. Subcutaneous omalizumab was started, with fast improvement of both symptoms and QoL score (from 3.9 up to 6.5). Seventeen months later, the dose of ICS had been gradually tapered and oral montelukast definitely discontinued. Currently, at age 14, treatment includes the combined administration of bimonthly subcutaneous omalizumab and of daily inhaled salmeterol/fluticasone (50 μg/100 μg∙day - 1 , respectively). Asthma control is satisfactory and no side effects are reported. Omalizumab has been continuously administered for 2.6 years and is still ongoing.
A full-term male had severe preschool wheezing and, since age 3, recurrent, severe asthma exacerbations with acute respiratory failure that frequently required intensive care unit (ICU) admission. At age 6, sensitization to multiple perennial inhalant (i.e., house dust mites, dog and cat danders, Alternaria alternata , Graminaceae pollen mix, Artemisia vulgaris , Parietaria judaica , and Olea europaea pollen) and food allergens (i.e., egg, milk, and peanut) was diagnosed. Serum IgE levels were 2219 KU/l. Weight and height were appropriate for age and sex. The patient has been treated over 3 years with a combined scheme of high-dose inhaled fluticasone (up to 1000 μg/day) plus salmeterol (100 μg/day) and oral montelukast (5 mg/day), with correct inhaler technique and good adherence. Despite this, monthly hospital admissions with systemic steroids use were recorded. Rhinosinusitis and GER were excluded on the basis of appropriate testing; thus treatment with omalizumab was started when the patient was 9 years old. At age 11, adherence to treatment is satisfactory, with no side effects. More importantly, reduced hospital admissions for asthma exacerbations, no further need for systemic steroids, and improved QoL score (from 6.4 to 6.8) were reported. Finally, progressive step-down of anti-asthma treatment was started, and at present (by 11.5 years) inhaled fluticasone (200 μg/day) plus bimonthly subcutaneous omalizumab provide good control of symptoms. Omalizumab has been continuously administered for 2.6 years and is still ongoing.
A full-term male had severe preschool wheezing and, since age 4, recurrent, severe asthma exacerbations with frequent hospital admissions. At age 8, multiple perennial inhalants and food sensitization (i.e., house dust mites, dog dander, Graminaceae pollen mix, Olea europaea pollen, tomatoes, beans, shrimps, and peas) and high serum IgE levels (1166 KU/l) were found. The patient has been treated over 5 years with inhaled fluticasone (up to 1000 μg/day) in association with salmeterol (100 μg/day) and oral montelukast (5 mg/day). Despite this, monthly hospital admissions with systemic steroids need were recorded. After checking the inhaler technique and adherence to treatment, comorbidities including obesity, rhinosinusitis and GER were excluded. Omalizumab was proposed, but parents refused it. By 13.6 years, despite a treatment including the association of inhaled salmeterol/fluticasone (100 μg/1000 μg∙day − 1 , respectively) plus oral montelukast (10 mg/day), monthly exacerbations requiring systemic steroids are reported.
Discussion and conclusions
Most children and adolescents with asthma respond well to inhaled short-acting beta 2 -agonists (SABA) on demand if symptoms are intermittent, or to low dose controller drugs plus as-needed SABA if the risk of exacerbations increases [ 1 ]. Nevertheless, a proportion of patients is referred to specialists because this strategy is not working and asthma is persistently uncontrolled [ 4 ]. For these children, assessment is primarily aimed at investigating the reasons for poor control. Indeed, when the child is initially referred, before the label of “severe, therapy-resistant asthma” (i.e., not responding to treatment even when factors as exposure to allergens and tobacco smoke have been considered) is assigned, three main categories need to be identified: 1) “not asthma at all”, in which response to treatment is suboptimal because the diagnosis is wrong; 2) “asthma plus ”, when asthma is mild but exacerbated by one or more comorbidities; and 3) “difficult-to-treat asthma”, when asthma is uncontrolled because of potentially reversible factors [ 10 ].
The reported cases highlight some aspects of the disease process that may expand the diagnosis and improve patients’ care. At our institution, the severe asthma program includes a multidisciplinary approach with consultations by gastroenterologists as well as ear, nose and throat experts. Recently, sleep medicine experts joined this multidisciplinary team; thus, unfortunately, sleep-disordered breathing (SDB) could not be excluded at the time of our patients’ assessment. Inhalation technique is periodically evaluated by nurses or doctors in each patient. Unfortunately, in Italy an individual prescription database is not available and thus we cannot assess patients’ use of medication. In two cases, the filtering process eventually identified GER and rhinosinusitis, but poor control of asthma persisted even after comorbidities were treated. In all subjects, inhaler skills, treatment adherence, and environmental exposure to indoor/outdoor allergens as well as to second- and third-hand smoke were excluded as cause of lack of control. Eventually, three out of four patients started anti-IgE treatment; asthma control was obtained and maintenance drugs were progressively reduced. In the case that refused omalizumab therapy, pulmonary function, clinical features and controller treatment including high-dose ICS were unchanged.
Previous studies have highlighted an association between increasing asthma severity in children and reduced QoL [ 11 , 12 , 13 ]. Uncontrolled asthma symptoms not only affect children physically, but can impair them socially, emotionally, and educationally [ 13 ]. In line with previous observations, 3 out 4 of our cases had poor QoL, assessed by a standardized questionnaire [ 14 ]. It is well known that improving QoL in difficult asthma is not an easy task, despite a variety of treatments aimed at achieving control [ 12 ], and much more remains to be done to address the problem. Nevertheless, 2 of our 3 cases showed a remarkable improvement of QoL after one year of treatment with omalizumab.
Reduction in forced expiratory volume in the first second (FEV 1 ) is often used to define childhood asthma severity in treatment guidelines and clinical studies [ 5 , 11 , 15 ]. Nevertheless, children with severe asthma often have a normal FEV 1 that does not improve after bronchodilators, indicating that spirometry may be a poor predictor of asthma severity in childhood [ 6 , 16 , 17 ]. Actually, children with a normal FEV 1 , both before and after β 2 -agonist, may show a bronchodilator response in terms of forced expiratory flow between 25% and 75% (FEF 25–75 ) [ 18 ]. However, the utility of FEF 25–75 in the assessment or treatment of severe asthma is currently unknown. Interestingly, all the reported cases showed normal or slightly reduced values of FEV 1 but severe impairment of FEF 25–75 . Two cases showed a bronchodilator response in terms of FEV 1 (subjects 3 and 4), while 3 patients had a significant increase of FEF 25–75 (cases 1, 3 and 4). Unfortunately, we could not provide the results of bronchodilator response during or after the treatment with omalizumab in any case.
Available literature on the diagnostic approach to difficult asthma in children offers a number of reviews which basically summarize the steps needed to fill the gap between a generic diagnosis of “difficult asthma” and more specific labels (i.e., “severe” asthma, “difficult-to-treat” asthma, or even different diagnoses) [ 3 , 5 , 6 , 8 , 10 , 19 , 20 , 21 ]. So far, few original articles and case reports have been published, probably due to the peculiarity of the issue, which makes retrospective discussion of cases easier than the design of a prospective clinical study [ 4 , 22 , 23 , 24 , 25 , 26 ]. Available knowledge mainly derives from the experience of specialized centers.
The evaluation of a child referred for uncontrolled asthma should start with a careful history focused on typical respiratory symptoms and on the definition of possible triggers. In the “severe asthma” process, it is crucial for clinicians to maintain a high degree of skepticism about the ultimate diagnosis, particularly in the presence of relevant discrepancies between history, physical features and lung function, as many conditions may be misdiagnosed as asthma. In order to simplify this process, herein we propose an algorithm for the diagnosis of difficult-to-treat and severe asthma (Fig. 1 ). Confirmation of the diagnosis through a detailed clinical and laboratory re-evaluation is important because in 12–50% of cases assumed to have severe asthma this might not be the correct diagnosis [ 10 ]. Several documents have indicated the main steps of the process that should be followed in children with uncontrolled asthma [ 3 , 8 , 10 ]. The translation of these procedures into real life practice may deeply change from one subject to another due to the variability of individual patients’ history and clinical features, which will often lead the diagnostic investigations towards the most likely reason for uncontrolled asthma. For children with apparently severe asthma, the first step is to confirm the diagnosis and, before proceeding to broader investigations, to verify that the poor control is not simply determined by poor adherence to treatment, inadequate inhaler skills and/or environmental exposure to triggers. A nurse-led assessment, including a home visit, despite not being applicable in all settings, may be useful for identifying potentially modifiable factors in uncontrolled pediatric asthma [ 27 ].
A practical algorithm for the diagnosis of difficult-to-treat and severe asthma. ICS, inhaled corticosteroids; OCS, oral corticosteroids
A number of comorbidities have been increasingly recognized as factors that may impact asthma clinical expression and control in childhood [ 10 , 28 ]. Children with uncontrolled disease should be investigated for GER, rhinosinusitis, dysfunctional breathing and/or vocal cord dysfunction, obstructive sleep apnea, obesity, psychological factors, smoke exposure, hormonal influences, and ongoing drugs [ 3 , 6 , 8 , 20 ]. Indeed, the exact role played by comorbidities in pediatric asthma control is still debated [ 28 ]. The most impressive example is GER. Several pediatric documents recommend assessing for GER because reflux may be a contributing factor to problematic or difficult asthma [ 7 , 29 ]. Nevertheless, GER treatment might not be effective for severe asthma [ 30 , 31 ], as confirmed by current cases 1 and 2. There is an established evidence that chronic rhinosinusitis is associated with more severe asthma in children [ 32 , 33 , 34 ]. Therefore, examination of upper airways and ad hoc treatment if rhinosinusitis is evident are recommended in children with severe asthma [ 3 , 8 , 35 ]. However, intranasal steroids for rhinitis resulted in a small reduction of asthma risk in school-aged children [ 36 ], and actual placebo-controlled studies on the effect of treatment of rhinosinusitis on asthma control in children are lacking [ 10 , 37 ].
Dysfunctional breathing, including hyperventilation and vocal cord dysfunction, is associated with poorer asthma control in children [ 8 , 10 , 38 , 39 ]. Unfortunately, there is scarce literature on the effect of its treatment on the control of severe asthma in children [ 40 ]. SDB ranging from primary snoring to obstructive sleep apnea syndrome is very common in children [ 41 ], and an increased prevalence of SDB together with increasing asthma severity has been reported [ 42 ]. Interestingly, GER may also be worsened by recurrent episodes of upper airway obstruction associated with SDB, and this may further trigger bronchial obstruction. Asthma guidelines recommend the assessment of SDB through nocturnal polysomnography in poorly controlled asthmatics, particularly if they are also obese [ 5 ]. There are no studies examining whether pediatric asthma improves after SDB has been treated, for example, with nasal steroids, adenotonsillectomy, continuous positive airway pressure or weight reduction if the child is also obese [ 43 ]. The parallel increase in obesity and asthma suggests that the two conditions are linked and that they can aggravate each other [ 44 , 45 ], even though the exact mechanisms that underlie this association remain unclear [ 46 ]. Indeed, other coexisting comorbidities such as SDB or GER may play a confounding role in the development of the interactions between obesity and the airways [ 47 , 48 ]. Obesity is associated with increased markers of inflammation in serum and adipose tissue and yet decreased airway inflammation in obese people with asthma [ 49 ]. Several interventions, including behavioral and weight reduction programs or bariatric surgery, may result in improved asthma control, quality of life and lung function in adult obese asthmatics [ 50 ]. Although reports of adolescent bariatric surgery demonstrate a significant body weight decrease, this approach is not widely available and there are no published reports on its effect on pediatric severe asthma control [ 51 ]. Finally, although it is still unclear whether food allergy is causative or shares a common pathway with difficult asthma, it might explain the loss of asthma control at least in some children and thus be considered as a comorbid condition [ 10 , 16 , 52 ].
In conclusion, establishing the impact of comorbidities on asthma control may be cumbersome, and an ex-juvantibus treatment is sometimes necessary to assess their role. Comorbid conditions can also worsen each other, and symptoms arising from some of them may mimic asthma [ 6 ]. Although the ability to improve pediatric severe asthma by treating comorbidities remains unconfirmed, they should be treated appropriately [ 9 ].
The vast majority of asthmatic children exhibit a mild or at most a moderate disease that can be fully controlled with low-to-medium dose ICS associated or not with other controllers [ 5 , 6 ]. However, a subset of asthmatics remains difficult-to-treat [ 5 , 6 ]. With the advent of biologics, these severe steroid-dependent asthmatics have alternative options for treatment, as steroid-related adverse events are common in severe asthma [ 53 ]. Omalizumab, an anti-IgE monoclonal antibody, is the only biologic therapy recommended in children with moderate-to-severe asthma by the recent guidelines [ 5 , 6 ]. In Italy, this treatment is fully covered by the National Health System. Therefore, there is no influence by any funding on treatment decisions. It was approved by the US (Food and Drug Administration) in 2003 and by the European Union (European Medicines Agency) in 2005 as an add-on treatment for patients aged > 12 years with severe persistent allergic asthma and who have a positive skin test or in-vitro reactivity to a perennial aeroallergen, FEV 1 < 80% predicted, frequent daytime symptoms or nighttime awakenings, and multiple documented severe asthma exacerbations despite daily ICS plus a LABA [ 54 , 55 ]. In 2009, it also received approval in Europe for treating patients aged 6–12 years. Figure 2 illustrates current indications for treatment with omalizumab in children and adolescents with severe asthma.
Indications for omalizumab in children and adolescents with severe asthma
IgE antibodies, Th 2 -derived cytokines and eosinophils play a major role in the development of chronic airway inflammation in asthmatic subjects [ 56 ]. Once released from plasma cells, IgE binds principally to the high-affinity IgE receptor (FcεRI) on mast cells, triggering different effector responses, including the release of mediators leading to allergic inflammatory reactions [ 56 ]. The activation of the allergic cascade by IgE, under constant allergen stimulation, leads to the establishment of chronic allergic inflammation in the airways of asthmatic patients, with IgE being a key element of the vicious circle that maintains it. Cytokines produced during the late phase and subsequent chronic inflammation stage have been directly associated with the induction of airway remodelling, indirectly implicating IgE in the process [ 56 ]. At present, omalizumab is the only commercially available recombinant humanized anti-IgE monoclonal antibody that specifically binds serum free IgE at its CH 3 domain, in the proximity of the binding site for FcεRI, thus preventing IgE from interacting with its receptor on mast cells, basophils, antigen-presenting cells and other inflammatory cells [ 57 ]. The rapid reduction of free IgE levels leads to a downregulation of the FcεRI expression on inflammatory cells and an interruption of the allergic cascade, which results in the reduction of peripheral and bronchial tissue eosinophilia and of levels of granulocyte macrophage colony stimulating factor, interleukin (IL)-2, IL-4, IL-5, and IL-13 [ 58 ]. Moreover, basophils have a relevant role in the initiation and progression of allergic inflammation, suggesting that they may represent a viable therapeutic target. Indeed, in children with severe asthma, it has been reported that omalizumab therapy is associated with a significant reduction in circulating basophil numbers, a finding that is concurrent with improved clinical outcomes [ 59 ]. This finding supports a mechanistic link between IgE levels and circulating basophil populations, and may provide new insights into one mechanism by which omalizumab improves asthma symptoms.
Several clinical controlled and real-life studies of adults with severe, inadequately controlled allergic asthma have demonstrated the efficacy and safety of omalizumab in reducing asthma-related symptoms, corticosteroid use, exacerbation rates, and healthcare resource utilization, and in improving QoL and lung function [ 60 , 61 , 62 , 63 ]. Fewer studies have been published in children. In two double-blind, randomized, placebo-controlled trials (RCTs) of children aged 6 to 12 years with moderate-to-severe allergic asthma, treatment with omalizumab reduced the requirement for ICS and protected against disease exacerbations, but there was little change in asthma symptom scores or spirometry [ 9 , 64 ]. These findings were confirmed and extended in older children [ 65 , 66 , 67 ].
The results of the ICATA study, a multicenter RCT of 419 inner-city children, adolescents and young adults with persistent allergic asthma, showed that, compared to placebo, omalizumab reduces the number of days with asthma symptoms and the proportion of participants with at least one exacerbation by approximately 25% and 19%, respectively ( p < 0.001), thus reducing the need for asthmatic symptom controllers [ 68 ]. Another multicenter RCT of inner-city children and adolescents showed that the addition of omalizumab to ongoing guidelines-based care before patients return to school reduces fall asthma exacerbations (odds ratio, 0.48), particularly in subjects with a recent exacerbation [ 69 ]. Moreover, in a real-life study of 104 children and adolescents with severe allergic refractory asthma followed over 1 year, treatment with omalizumab resulted in good asthma control in 67% of the cases ( p < 0.001), while FEV 1 improved by 4.9% ( p = 0.02) and exacerbation rates and healthcare utilisation decreased approximately by 30% ( p < 0.001) [ 70 ]. The same authors also showed that, after two years of treatment, exacerbation rate and healthcare utilisation were further decreased by 83% and 100%, respectively, while level of asthma control, steroid use and lung function remained unchanged [ 71 ].
A systematic review of pediatric RCTs pooled the data of 1381 children and adolescents with moderate-to-severe allergic asthma in order to establish the efficacy of omalizumab as an add-on therapy [ 72 ]. During the stable-steroid phase, omalizumab decreased the number of patients with at least one exacerbation (risk ratio, 0.69; p < 0.001), the mean number of asthma exacerbations per patient (risk ratio, 0.35; p < 0.001), and the asthma symptom score (mean difference, 0.12; p = 0.005) when compared to placebo. During the steroid reduction phase, omalizumab further reduced the number of patients with at least one exacerbation (risk ratio, 0.48; p < 0.001) and the mean number of asthma exacerbations per patient (mean difference, 0.12; p < 0.05).
Given the cost of omalizumab, many authors have argued for the importance of identifying specific asthma populations who will have significant benefit from it [ 68 , 73 , 74 ]. In the ICATA study, baseline predictors of good response to treatment were sensitization and exposure to cockroach allergen, sensitization to house dust mite allergens, a serum IgE level of more than 100 IU per milliliter, a BMI of 25 or more, and a history of at least one unscheduled medical visit in the previous year [ 68 ].
Several studies have assessed the long-term safety of omalizumab in children and adults. A pooled analysis of 67 RCTs conducted over 2 decades on 4254 children and adults treated with omalizumab showed no association between omalizumab treatment and risk of malignancy [ 75 ]. In an RCT evaluating 225 school-aged children, omalizumab was well tolerated, there were no serious adverse events, and the frequency and types of all adverse events were similar to the placebo group [ 9 ]. These results have been further confirmed by a recent systematic review of RCTs that concluded that treatment with omalizumab does not result in increased risk of malignancy or hypersensitivity reactions [ 72 ].
While the rationale for long-term treatment with omalizumab is supported by pharmacokinetic-pharmacodynamic models [ 76 ], the duration of treatment is still under discussion. Results from published studies suggest that omalizumab should be continued for > 1 year [ 77 , 78 ]. In a retrospective study of adults and children with uncontrolled severe asthma treated with omalizumab, the response to treatment was ‘excellent’ in 52.5% of patients, particularly in the subgroup of children aged 6 to 11 years [ 77 ]. After the discontinuation of treatment, loss of asthma control was documented in 69.2% of the patients who had received omalizumab for < 1 year, 59.1% of the subjects treated for 1–2 years, and 46.1% of the cases treated for > 2 years. Time to loss of control was shorter in younger children and longer in patients with an ‘excellent’ response compared with patients with a ‘good’ response. No early loss of control (within 6 months) was observed among patients with > 3.5 years of continuous treatment with omalizumab. Finally, 20% of patients in whom omalizumab was re-prescribed because of loss of control did not respond to the treatment anymore [ 77 ]. Despite these encouraging findings, the impact of omalizumab on the natural history of severe asthma in children deserves to be further investigated by long-term studies that will also define the criteria and timing for discontinuing the treatment.
It is well known that asthma pharmacotherapy is effective in controlling symptoms and bronchial inflammation, but cannot affect the underlying immune response, thus leading to the possibility of symptom reappearance after its discontinuation [ 79 ]. In this scenario, allergen-specific immunotherapy (AIT) has been proposed as the only therapeutic method that can modulate the underlying immune pathophysiology in allergic asthma [ 80 ].
AIT is currently indicated in children and adults with mild-moderate allergic asthma that is completely or partially controlled by pharmacotherapy and with the evidence of a clear relationship between symptoms and exposure to a specific allergen [ 81 , 82 , 83 , 84 ]. However, according to recent guidelines, the efficacy of AIT in asthmatic subjects is limited, and its potential benefits must be weighed against the risk of side effects and the inconvenience and costs of the prolonged therapy [ 5 ]. Moreover, severe or uncontrolled asthma (regardless of its severity) is a major independent risk factor for non-fatal or even fatal adverse reactions, thus representing a contraindication for AIT [ 85 , 86 , 87 ]. Finally, children with severe asthma are often sensitized to multiple allergens, thus making AIT prescription even more complicated [ 88 ].
In subjects with uncontrolled and/or severe allergic asthma, a combination of omalizumab and AIT has been proposed [ 88 ]. Surprisingly, only a few studies have addressed this issue [ 89 , 90 , 91 , 92 ]. However, pre-treatment with omalizumab seems to improve the efficacy and tolerability of subcutaneous AIT in children and adults with severe allergic asthma both during omalizumab treatment and after its discontinuation [ 89 , 91 , 92 ]. Omalizumab has also been successfully used as a supplementary treatment to AIT in order to improve asthma control in children ≥6 years with severe persistent allergic asthma [ 90 ]. Given the scarcity of studies on AIT plus omalizumab in children with severe allergic asthma, further research is warranted to assess risks and benefits of the combined treatment.
Children with severe asthma require a detailed and individualized approach including re-assessment for differential diagnoses, comorbidities and contributory factors, environmental triggers, lung function and inflammation, adherence and response to therapy, and QoL. Treatment of pediatric severe asthma still relies on the maximal optimal use of corticosteroids, bronchodilators and other controllers recommended for moderate-to-severe disease. However, the management of asthma is becoming much more patient-specific, as more and more is learned about the biology behind the development and progression of asthma.
In the current paper, we described the characteristics of four children with severe asthma in whom omalizumab was prescribed. A review of the relevant literature on the topic was also performed. Finally, we provided an algorithm for the diagnosis of difficult-to-treat and severe asthma in children and adolescents, based on the evidence from the literature review. As all algorithms, it is not meant to replace clinical judgment, but it should drive physicians to adopt a systematic approach towards difficult and severe asthma and provide a useful guide to the clinician.
The addition of omalizumab, the first targeted biological treatment approved for asthma, has led to renewed optimism of outcome improvements in patients with allergic severe asthma. As severe asthma is a heterogeneous condition consisting of different phenotypes, the future of asthma management will likely involve phenotypic and potentially even genotypic characterization in selected cases in order to determine appropriate therapy and thus to provide the highest possible benefit, especially if specific responder phenotypes can be identified and selected for this highly specific treatment.
Abbreviations
Anti-immunoglobulin E
Body mass index
IgE receptor
Forced expiratory flow between 25% and 75%
Forced expiratory volume in the first second
Gastroesophageal reflux
Inhaled corticosteroids
Intensive care unit
Interleukin
Long-acting β 2 -agonist
Oral leukotriene receptor antagonist
Quality of life
Randomized controlled trials
Short-acting β 2 -agonists
Sleep-disordered breathing
O'Byrne PM, Pedersen S, Schatz M, Thoren A, Ekholm E, Carlsson LG, et al. The poorly explored impact of uncontrolled asthma. Chest. 2013;143:511–3.
Article PubMed Google Scholar
National Asthma Education and Prevention Program. Expert panel report 3 (EPR-3): guidelines for the diagnosis and Management of Asthma-Summary Report 2007. J Allergy Clin Immunol. 2007;120:S94–8.
Article Google Scholar
Hedlin G. Management of severe asthma in childhood-state of the art and novel perspectives. Pediatr Allergy Immunol. 2014;25:111–21.
Konradsen JR, Nordlund B, Lidegran M, Pedroletti C, Grönlund H, van Hage M, et al. Problematic severe asthma: a proposed approach to identifying children who are severely resistant to therapy. Pediatr Allergy Immunol. 2011;22:9–18.
Global Initiative for Asthma Report. Global strategy for asthma management and prevention (updated 2016). https://www.ginasthma.org . Accessed 07 June 2017.
Chung KF, Wenzel SE, Brozek JL, Bush A, Castro M, Sterk PJ, et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur Respir J. 2014;43:343–53.
Article CAS PubMed Google Scholar
Vandenplas Y, Rudolph CD, Di Lorenzo C, Hassall E, Liptak G, Mazur L, et al. Pediatric gastroesophageal reflux clinical practice guidelines: joint recommendations of the north American Society for Pediatric Gastroenterology, Hepatology, and nutrition (NASPGHAN) and the European Society for Pediatric Gastroenterology, Hepatology, and nutrition (ESPGHAN). J Pediatr Gastroenterol Nutr. 2009;49:498–507.
Lødrup Carlsen KC, Hedlin G, Bush A, Wennergren G, de Benedictis FM, De Jongste JC, et al. Assessment of problematic severe asthma in children. Eur Respir J. 2011;37:432–40.
Milgrom H, Berger W, Nayak A, Gupta N, Pollard S, McAlary M, et al. Treatment of childhood asthma with anti-immunoglobulin E antibody (omalizumab). Pediatrics. 2001;108:E36.
Bush A, Saglani S. Management of severe asthma in children. Lancet. 2010;376:814–5.
Article CAS PubMed PubMed Central Google Scholar
Lang A, Mowinckel P, Sachs-Olsen C, Riiser A, Lunde J, Carlsen KH, et al. Asthma severity in childhood, untangling clinical phenotypes. Pediatr Allergy Immunol. 2010;21:945–53.
Nordlund B, Konradsen JR, Pedroletti C, Kull I, Hedlin G. The clinical benefit of evaluating health-related quality-of-life in children with problematic severe asthma. Acta Paediatr. 2011;100:1454–60.
Dean BB, Calimlim BC, Sacco P, Aguilar D, Maykut R, Tinkelman D. Uncontrolled asthma: assessing quality of life and productivity of children and their caregivers using a cross-sectional internet-based survey. Health Qual Life Outcomes. 2010;8:6.
Juniper EF, Guyatt GH, Feeny DH, Ferrie PJ, Griffith LE, Townsend M. Measuring quality of life in children with asthma. Qual Life Res. 1996;5:35–46.
British Thoracic Society. Scottish Intercollegiate Guidelines Network. British guideline on the management of asthma, 2014. https://www.brit-thoracic.org.uk/guidelines-and-quality-standards/asthma-guideline . Accessed 13 Apr 2016.
Montella S, Baraldi E, Cazzato S, Aralla R, Berardi M, Brunetti LM, et al. Severe asthma features in children: a case-control online survey. Ital J Pediatr. 2016;42:9.
Article PubMed PubMed Central Google Scholar
Fitzpatrick AM, Gaston BM, Erzurum SC, Teague WG, National Institutes of Health/National Heart, Lung, and Blood Institute Severe Asthma Research Program. Features of severe asthma in school-age children: Atopy and increased exhaled nitric oxide. J Allergy Clin Immunol. 2006;118:1218–25.
Simon MR, Chinchilli VM, Phillips BR, Sorkness CA, Lemanske RF Jr, Szefler SJ, et al. Forced expiratory flow between 25% and 75% of vital capacity and FEV1/forced vital capacity ratio in relation to clinical and physiological parameters in asthmatic children with normal FEV1 values. J Allergy Clin Immunol. 2010;126:527–34.
Hedlin G, Bush A, Lødrup Carlsen K, Wennergren G, De Benedictis FM, Melén E, et al. Problematic severe asthma in children, not one problem but many: a GA2LEN initiative. Eur Respir J. 2010;36:196–201.
Fitzpatrick AM, Teague WG. Severe asthma in children: insights from the National Heart, Lung, and Blood Institute's severe asthma research program. Pediatr Allergy Immunol Pulmonol. 2010;23:131–8.
Konradsen JR, Caffrey Osvald E, Hedlin G. Update on the current methods for the diagnosis and treatment of severe childhood asthma. Expert Rev Respir Med. 2015;9:769–77.
Lang AM, Konradsen J, Carlsen KH, Sachs-Olsen C, Mowinckel P, Hedlin G, et al. Identifying problematic severe asthma in the individual child—does lung function matter? Acta Paediatr. 2010;99:404–10.
Rao DR, Gaffin JM, Baxi SN, Sheehan WJ, Hoffman EB, Phipatanakul WJ. The utility of forced expiratory flow between 25% and 75% of vital capacity in predicting childhood asthma morbidity and severity. Asthma. 2012;49:586–92.
Eid N, Yandell B, Howell L, Eddy M, Sheikh S. Can peak expiratory flow predict airflow obstruction in children with asthma? Pediatrics. 2000;105:354–8.
Cicutto LC, Chapman KR, Chamberlain D, Downey GP. Difficult asthma: consider all of the possibilities. Can Respir J. 2000;7:415–8.
Wener RR, Bel EH. Severe refractory asthma: an update. Eur Respir Rev. 2013;22:227–35.
Bracken M, Fleming L, Hall P, et al. The importance of nurse-led home visits in the assessment of children with problematic asthma. Arch Dis Child. 2009;94:780–4.
De Groot EP, Kreggemeijer WJ, Brand PL. Getting the basics right resolves most cases of uncontrolled and problematic asthma. Acta Paediatr. 2015;104:916–21.
Grimaldi-Bensouda L, Zureik M, Aubier M, Humbert M, Levy J, Benichou J, et al. Does omalizumab make a difference to the real-life treatment of asthma exacerbations? Results from a large cohort of patients with severe uncontrolled asthma. Chest. 2013;143:398–405.
American Lung Association Asthma Clinical Research Centers, Mastronarde JG, Anthonisen NR, Castro M, Holbrook JT, Leone FT, et al. Efficacy of esomeprazole for treatment of poorly controlled asthma. N Engl J Med. 2009;360:1487–9.
Article PubMed Central Google Scholar
Writing Committee for the American Lung Association Asthma Clinical Research Centers, Holbrook JT, Wise RA, Gold BD, Blake K, Brown ED, et al. Lansoprazole for children with poorly controlled asthma: a randomized controlled trial. JAMA 2012;307:373-381.
Wright AL, Holberg CJ, Martinez FD, Halonen M, Morgan W, Taussig LM. Epidemiology of physician-diagnosed allergic rhinitis in childhood. Pediatrics. 1994;94:895–901.
CAS PubMed Google Scholar
De Groot EP, Nijkamp A, Duiverman EJ, Brand PL. Allergic rhinitis is associated with poor asthma control in children with asthma. Thorax. 2012;67:582–7.
Rotiroti G, Roberts G, Scadding GK. Rhinitis in children: common clinical presentations and differential diagnoses. Pediatr Allergy Immunol. 2015;26:103–10.
Bousquet J, Khaltaev N, Cruz AA, Denburg J, Fokkens WJ, Togias A, et al. Allergic rhinitis and its impact on asthma (ARIA). 2008 update (in collaboration with the World Health Organization, GA(2)LEN and AllerGen). Allergy. 2008;63:S8–160.
Deliu M, Belgrave D, Simpson A, Murray CS, Kerry G, Custovic A. Impact of rhinitis on asthma severity in school-age children. Allergy. 2014;69:1515–21.
Brozek JL, Bousquet J, Baena-Cagnani CE, Bonini S, Canonica GW, Casale TB, et al. Allergic rhinitis and its impact on asthma (ARIA) guidelines: 2010 revision. J Allergy Clin Immunol. 2010;126:466–76.
Weinberger M, Abu-Hasan M. Pseudo-asthma: when cough, wheezing, and dyspnea are not asthma. Pediatrics. 2007;120:855–64.
De Groot EP, Duiverman EJ, Brand PL. Dysfunctional breathing in children with asthma: a rare but relevant comorbidity. Eur Respir J. 2013;41:1068–73.
Barker NJ, Jones M, O'Connell NE, Everard ML. Breathing exercises for dysfunctional breathing/hyperventilation syndrome in children. Cochrane Database Syst Rev. 2013;12:CD010376.
Google Scholar
Section on Pediatric Pulmonology, Subcommittee on Obstructive Sleep Apnea Syndrome, American Academy of Pediatrics. Clinical practice guideline: diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics. 2002;109:704–12.
Goldstein NA, Aronin C, Kantrowitz B, Hershcopf R, Fishkin S, Lee H, Weaver DE, et al. The prevalence of sleep-disordered breathing in children with asthma and its behavioral effects. Pediatr Pulmonol. 2015;50:1128–36.
Ross KR, Storfer-Isser A, Hart MA, Kibler AM, Rueschman M, Rosen CL, et al. Sleep-disordered breathing is associated with asthma severity in children. J Pediatr. 2012;160:736–42.
Santamaria F, Montella S, Greco L, Valerio G, Franzese A, Maniscalco M, et al. Obesity duration is associated to pulmonary function impairment in obese subjects. Obesity (Silver Spring). 2011;19:1623–8.
Sivapalan P, Diamant Z, Ulrik CS. Obesity and asthma: current knowledge and future needs. Curr Opin Pulm Med. 2015;21:80–5.
Rasmussen F, Hancox RJ. Mechanisms of obesity in asthma. Curr Opin Allergy Clin Immunol. 2014;14:35–43.
Santamaria F, Montella S, Pietrobelli A. Obesity and pulmonary disease: unanswered questions. Obes Rev. 2012;13:822–33.
Lang JE, Hossain J, Holbrook JT, Teague WG, Gold BD, Wise RA, et al. Gastro-oesophageal reflux and worse asthma control in obese children: a case of symptom misattribution? Thorax. 2016;71:238–46.
Santamaria F, Montella S, De Stefano S, Sperlì F, Barbarano F, Valerio G. Relationship between exhaled nitric oxide and body mass index in children and adolescents. J Allergy Clin Immunol. 2005;116:1163–4.
Van Huisstede A, Rudolphus A, Castro Cabezas M, Biter LU, van de Geijn GJ, Taube C, et al. Effect of bariatric surgery on asthma control, lung function and bronchial and systemic inflammation in morbidly obese subjects with asthma. Thorax. 2015;70:659–67.
Katzmarzyk PT, Bouchard C. Where is the beef? Waist circumference is more highly correlated with BMI and total body fat than with abdominal visceral fat in children. Int J Obes. 2014;38:753–4.
Article CAS Google Scholar
De Groot EP, Duiverman EJ, Brand PL. Comorbidities of asthma during childhood: possibly important, yet poorly studied. Eur Respir J. 2010;36:671–8.
Sweeney J, Patterson CC, Menzies-Gow A, Niven RM, Mansur AH, Bucknall C, et al. Comorbidity in severe asthma requiring systemic corticosteroid therapy: cross-sectional data from the optimum patient care research database and the British thoracic difficult asthma registry. Thorax. 2016; https://doi.org/10.1136/thoraxjnl-2015-207630 .
Federal Drug Administration Advisory for Omalizumab. Available at: https://wayback.archive-it.org/7993/20170111075347/ . http://www.fda.gov/Drugs/DevelopmentApprovalProcess/HowDrugsareDevelopedandApproved/ApprovalApplications/TherapeuticBiologicApplications/default.htm . Accessed 4 Feb 2018.
European Medicines Agency: assessment report for Xolair. Available at: http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/medicines/000606/human_med_001162.jsp&mid=WC0b01ac058001d124 . Accessed 7 June 2017.
Chung KF. Targeting the interleukin pathway in the treatment of asthma. Lancet. 2015;386:1086–96.
Jensen RK, Plum M, Tjerrild L, Jakob T, Spillner E, Andersen GR. Structure of the omalizumab Fab. Acta Crystallogr F Struct Biol Commun. 2015;71:419–26.
Holgate S, Smith N, Massanari M, Jimenez P. Effects of omalizumab on markers of inflammation in patients with allergic asthma. Allergy. 2009;64:1728–36.
Hill DA, Siracusa MC, Ruymann KR, Tait Wojno ED, Artis D, Spergel JM. Omalizumab therapy is associated with reduced circulating basophil populations in asthmatic children. Allergy. 2014;69:674–7.
Humbert M, Beasley R, Ayres J, Slavin R, Hébert J, Bousquet J, et al. Benefits of omalizumab as add-on therapy in patients with severe persistent asthma who are inadequately controlled despite best available therapy (GINA 2002 step 4 treatment): INNOVATE. Allergy. 2005;60:309–16.
Normansell R, Walker S, Milan SJ, Walters EH, Nair P. Omalizumab for asthma in adults and children. Cochrane Database Syst Rev. 2014;1:CD003559.
Lai T, Wang S, Xu Z, Zhang C, Zhao Y, Hu Y, Cao C, et al. Long-term efficacy and safety of omalizumab in patients with persistent uncontrolled allergic asthma: a systematic review and meta-analysis. Sci Rep. 2015;5:8191.
Abraham I, Alhossan A, Lee CS, Kutbi H, MacDonald K. “real-life” effectiveness studies of omalizumab in adult patients with severe allergic asthma: systematic review. Allergy. 2015; https://doi.org/10.1111/all.12815 .
Lanier B, Bridges T, Kulus M, Taylor AF, Berhane I, Vidaurre CF. Omalizumab for the treatment of exacerbations in children with inadequately controlled allergic (IgE-mediated) asthma. J Allergy Clin Immunol. 2009;124:1210–6.
Solèr M, Matz J, Townley R, Buhl R, O'Brien J, Fox H, et al. The anti-IgE antibody omalizumab reduces exacerbations and steroid requirement in allergic asthmatics. Eur Respir J. 2001;18:254–61.
Holgate ST. Cytokine and anti-cytokine therapy for the treatment of asthma and allergic disease. Cytokine. 2004;28:152–7.
Odajima H, Ebisawa M, Nagakura T, Fujisawa T, Akasawa A, Ito K, et al. Omalizumab in Japanese children with severe allergic asthma uncontrolled with standard therapy. Allergol Int. 2015;64:364–70.
Busse WW, Morgan WJ, Gergen PJ, Mitchell HE, Gern JE, Liu AH, et al. Randomized trial of omalizumab (anti-IgE) for asthma in inner-city children. N Engl J Med. 2011;364:1005–15.
Teach SJ, Gill MA, Togias A, Sorkness CA, Arbes SJ Jr, Calatroni A, et al. Preseasonal treatment with either omalizumab or an inhaled corticosteroid boost to prevent fall asthma exacerbations. J Allergy Clin Immunol. 2015;136:1476–85.
Deschildre A, Marguet C, Salleron J, Pin I, Rittié JL, Derelle J, et al. Add-on omalizumab in children with severe allergic asthma: a 1-year real life survey. Eur Respir J. 2013;42:1224–33.
Deschildre A, Marguet C, Langlois C, Pin I, Rittié JL, Derelle J, et al. Real-life long-term omalizumab therapy in children with severe allergic asthma. Eur Respir J. 2015;46:856–9.
Rodrigo GJ, Neffen H. Systematic review on the use of omalizumab for the treatment of asthmatic children and adolescents. Pediatr Allergy Immunol. 2015;26:551–6.
Oba Y, Salzman GA. Cost-effectiveness analysis of omalizumab in adults and adolescents with moderate-to-severe allergic asthma. J Allergy Clin Immunol. 2004;114:265–9.
Campbell JD, Spackman DE, Sullivan SD. The costs and consequences of omalizumab in uncontrolled asthma from a USA payer perspective. Allergy. 2010;65:1141–8.
Busse W, Buhl R, Fernandez Vidaurre C, Blogg M, Zhu J, Eisner MD, et al. Omalizumab and the risk of malignancy: results from a pooled analysis. J Allergy Clin Immunol. 2012;129:983–9.
Lowe PJ, Renard D. Omalizumab decreases IgE production in patients with allergic (IgE-mediated) asthma; PKPD analysis of a biomarker, total IgE. Br J Clin Pharmacol. 2011;72:306–10.
Molimard M, Mala L, Bourdeix I, Le Gros V. Observational study in severe asthmatic patients after discontinuation of omalizumab for good asthma control. Respir Med. 2014;108:571–6.
Busse WW, Trzaskoma B, Omachi TA, Canvin J, Rosen K, Chipps BE, et al. Evaluating Xolair persistency of response after long-term therapy (XPORT). Am J Respir Crit Care Med. 2014;189:A6576.
Guilbert TW, Morgan WJ, Zeiger RS, Mauger DT, Boehmer SJ, Szefler SJ, et al. Long-term inhaled corticosteroids in preschool children at high risk for asthma. N Engl J Med. 2006;354:1985–97.
Akdis CA. Therapies for allergic inflammation: refining strategies to induce tolerance. Nat Med. 2012;18:736–49.
National Heart, Lung, and Blood Institute. Expert panel report 3: Guidelines for the diagnosis and management of asthma—full report 2007. Available at: https://www.nhlbi.nih.gov/files/docs/guidelines/asthgdln.pdf . Accessed 4 Feb 2018.
Joint Task Force on Practice Parameters, American Academy of Allergy, Asthma and Immunology, American College of Allergy, Asthma and Immunology, Joint Council of Allergy, Asthma and Immunolgy. Allergen immunotherapy: a practice parameter second update. J Allergy Clin Immunol. 2007;120:S25–85.
Zuberbier T, Bachert C, Bousquet PJ, Passalacqua G, Walter Canonica G, Merk H, et al. GA(2) LEN/EAACI pocket guide for allergen-specific immunotherapy for allergic rhinitis and asthma. Allergy. 2010;65:1525–30.
Pajno GB, Bernardini R, Peroni D, Arasi S, Martelli A, Landi M, et al. Clinical practice recommendations for allergen-specific immunotherapy in children: the Italian consensus report. Ital J Pediatr. 2017;43:13.
Pitsios C, Demoly P, Bilo MB, Gerth van Wijk R, Pfaar O, Sturm GJ, et al. Clinical contraindications to allergen immunotherapy: an EAACI position paper. Allergy. 2015;70:897–909.
Tsabouri S, Mavroudi A, Feketea G, Guibas GV. Subcutaneous and sublingual immunotherapy in allergic asthma in children. Front Pediatr. 2017;5:82.
Jutel M, Agache I, Bonini S, Burks AW, Calderon M, Canonica W, et al. International consensus on allergy immunotherapy. J Allergy Clin Immunol. 2015;136:556–68.
Hedlin G, van Hage M. The role of immunotherapy in the management of childhood asthma. Ther Adv Respir Dis. 2012;6:137–46.
Lambert N, Guiddir T, Amat F, Just J. Pre-treatment by omalizumab allows allergen immunotherapy in children and young adults with severe allergic asthma. Pediatr Allergy Immunol. 2014;25:829–32.
Kopp MV, Hamelmann E, Zielen S, Kamin W, Bergmann K-C, Sieder C. Combination of omalizumab and specific immunotherapy is superior to immunotherapy in patients with seasonal allergic rhinoconjunctivitis and co-morbid seasonal allergic asthma. Clin Exp Allergy. 2009;39:271–9.
Massanari M, Nelson H, Casale T, Busse W, Kianifard F, Geba GP. Effect of pretreatment with omalizumab on the tolerability of specific immunotherapy in allergic asthma. J Allergy Clin Immunol. 2010;125:383–9.
Stelmach I, Kaczmarek-Woźniak J, Majak P, Olszowiec-Chlebna M, Jerzynska J. Efficacy and safety of high-doses sublingual immunotherapy in ultra-rush scheme in children allergic to grass pollen. Clin Exp Allergy. 2009;39:401–8.
Download references
Acknowledgements
The authors gratefully thank Dr. Marco Maglione for his contribution in the clinical assessment of the described cases. Medical writing assistance was provided by Stephen Walters on behalf of City Hills Proofreading.
No funding was secured for this study.
Availability of data and materials
All relevant data and materials are published in the manuscript.
Author information
Authors and affiliations.
Department of Translational Medical Sciences, Federico II University, Via Sergio Pansini 5, 80131, Naples, Italy
Virginia Mirra, Silvia Montella & Francesca Santamaria
You can also search for this author in PubMed Google Scholar
Contributions
VM, SM and FS, authors of the current manuscript, declare that they have participated sufficiently in the work to take public responsibility for appropriate portions of the content. VM and SM carried out the initial investigations, drafted the initial manuscript, revised the manuscript, and approved the final manuscript as submitted. FS conceptualized and designed the study, and critically reviewed and approved the final manuscript as submitted. All authors read and approved the final manuscript.
Corresponding author
Correspondence to Francesca Santamaria .
Ethics declarations
Ethics approval and consent to participate.
This study was approved by the ethics committee “Carlo Romano”, Federico II University, Naples, Italy. Children’s parents/legal guardians gave informed written consent to participate. The description of our cases adheres to the CARE standards of reporting checklist.
Consent for publication
Children’s parents/legal guardians provided informed written consent for the case report to be published.
Competing interests
The authors declare that they have no competing interests to disclose. Authors have no financial relationships relevant to this article to disclose.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License ( http://creativecommons.org/licenses/by/4.0/ ), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated.
Reprints and permissions
About this article
Cite this article.
Mirra, V., Montella, S. & Santamaria, F. Pediatric severe asthma: a case series report and perspectives on anti-IgE treatment. BMC Pediatr 18 , 73 (2018). https://doi.org/10.1186/s12887-018-1019-9
Download citation
Received : 24 May 2016
Accepted : 29 January 2018
Published : 21 February 2018
DOI : https://doi.org/10.1186/s12887-018-1019-9
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Severe asthma
- Adolescents
- Asthma exacerbations
BMC Pediatrics
ISSN: 1471-2431
- General enquiries: [email protected]

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
Case Study: A Patient with Asthma, Covid-19 Pneumonia and Cytokine Release Syndrome Treated with Corticosteroids and Tocilizumab
Gunter k schleicher.
1 Department of Critical Care and Pulmonology, Wits Donald Gordon Medical Centre, Johannesburg, South Africa
Warren Lowman
2 Pathcare/Vermaak Laboratories, Department of Clinical Microbiology and Infectious Diseases, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
Guy A Richards
3 Department of Internal Medicine, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
INTRODUCTION
Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) is the novel coronavirus first detected in Wuhan, China, that causes coronavirus disease 2019 (Covid-19) and pneumonia. Covid-19 pneumonia is defined by a positive result for SARS-CoV-2 on a reverse-transcriptase–polymerase-chain-reaction (RT-PCR) assay of a specimen collected from the upper or lower respiratory tract together with radiological features of pneumonia and clinical features of hypoxaemia and dyspnoea. Although more than 80% of patients with Covid-19 infection have mild disease and make a full recovery, a significant proportion of patients progress to pneumonia, and about half of these cases will develop severe acute respiratory syndrome (ARDS). Initial reports from China suggested that age >65 years and medical comorbidities are risk factors for poor outcomes.( 1 ) The need for ICU admission and mechanical ventilation once ARDS develops is associated with a high mortality, ranging from 39% to 72%.( 2 , 3 ) Current guidelines recommend that corticosteroids or immunosuppressive therapy should not be used in patients with Covid-19 pneumonia unless there are other indications, such as shock, asthma or exacerbation of chronic obstructive pulmonary disease.( 4 ) However, the role of systemic corticosteroids is currently being re-evaluated in mechanically ventilated adults with ARDS, with some guidelines now suggesting their use.( 5 )
We describe a case of a patient with Covid-19 infection, progressive pneumonia, development of a hyperinflammatory state and cytokine release syndrome (CRS) who was successfully treated with steroids and tocilizumab.
CASE REPORT
In January 2020, a 53-year-old gentleman with a background of asthma on long-term low dose inhaled corticosteroid inhaler had an acute exacerbation of his asthma in February 2020 triggered by a viral upper respiratory tract infection and acute sinusitis and was managed with bronchodilator nebulization and a 7-day course of oral prednisone 30 mg daily. He made an uneventful recovery and proceeded to travel to Austria on 29 February 2020. During his stay in Austria, he had contact with a Covid-19 positive individual and started developing upper respiratory symptoms on 7 March. On his return to South Africa on 8 March he had a fever, sore throat, dry cough, severe wheezing and worsening dyspnoea. At that stage a commercial test for Covid-19 PCR was not yet available to the private pathology laboratories and blood tests showed a normal full blood count and a C-reactive protein (CRP) of 16 mg/L. He was advised to self-isolate at home and was managed telephonically with bronchodilator nebulization, oral prednisone 30 mg daily for 5 days and paracetamol. By 11 March he was not feeling any better and had ongoing fever and cough. The Covid-19 PCR test had become available at that stage and his initial test with a private pathology laboratory was negative.
Over the next 3 days his symptoms worsened, and on 16 March he was admitted to hospital to an isolation ward where blood tests showed a lymphopaenia and a rising CRP ( Table 1 ). A high-resolution CT scan of his chest showed bilateral asymmetrical peripheral ground glass infiltrates in a subsegmental distribution, particularly in the lower zones. A repeat Covid-19 PCR swab on this occasion was positive and he was diagnosed with Covid-19 pneumonia. His oxygen saturation was 86% on room air. He was haemodynamically stable and was kept in strict isolation, and treatment was commenced with supplemental oxygen via a nasal cannula, paracetamol, chloroquine, azithromycin and lopinavir/ritonavir. In keeping with national and international guidelines recommending against the use of systemic corticosteroids, prednisone was discontinued.
Laboratory and pathology results during hospital admission and post discharge
| Date | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| 2020-03-16 | 2020-03-17 | 2020-03-21 | 2020-03-23 | 2020-03-24 | 2020-03-25 | 2020-03-26 | 2020-03-27 | 2020-03-31 | |
| Laboratory marker | |||||||||
| White cell count (4–10 × 10 /L) | 7.0 | 6.1 | 9,6 | 7,6 | 9.5 | 8.1 | 6.3 | 6.6 | 9.0 |
| Neutrophils abs (2–7 × 10 /L) | 5.8 | 4.2 | 8,9 | 7,3 | 8.4 | 6.4 | 4.3 | 4.6 | 6.9 |
| Lymphocytes abs (1–3 × 10 /L) | 0.6 | 1.2 | 0,4 | 0,2 | 0.6 | 1.1 | 1.3 | 1.2 | 1.4 |
| Neutrophil: Lymphocyte ratio | 9.6 | 3.5 | 22,3 | 36,5 | 14.0 | 5.8 | 3.3 | 3.8 | 5.1 |
| CRP (0–10 mg/L) | 56 | 73 | 98 | 169 | 94 | 43 | 22 | 12 | 4 |
| PCT (0–0.05 ng/L) | 0,05 | 0,04 | 0.03 | 0.02 | 0.04 | ||||
| Ferritin (22–275 μg/L | 1900 | 1951 | 1164 | ||||||
| LDH (125–220 U/L) | 185 | 161 | 340 | 259 | 235 | ||||
| D-Dimer (0–0.225 mg/L) | 0,37 | 1,11 | 0.85 | 0.86 | 0.66 | ||||
| Pro-BNP`(<125 ng/L) | 338 | 297 | 173 | 115 | 98 | ||||
| SARS-CoV-2 | Detected | Not detected | |||||||
| ↑ | ↑ | ||||||||
| Tocilizumab | Tocilizumab | ||||||||
Arrows indicate treatment with tocilizumab 400 mg IV.
Over the next 5 days his clinical condition worsened despite antiviral therapy. His biomarkers, including lymphopaenia, CRP, pro-B-type natriuretic peptide (Pro-BNP), lactate dehydrogenase (LDH), D-dimers and ferritin all increased significantly ( Table 1 ). His hypoxaemia worsened and he had increased bilateral chest infiltrates on follow-up radiology ( Figure 1 ). His PaO2:FiO2 ratio decreased to 250. He was diagnosed as having Covid-19 hyperinflammatory syndrome, CRS and ARDS. After a discussion with the team he was treated with tocilizumab 800 mg IV, given as two doses of 400 mg 24 h apart on 23 and 24 March, as well as methylprednisolone 40 mg IV daily for 5 days. Chloroquine dose was reduced, and azithromycin and lopinavir/ritonavir were discontinued in view of QT prolongation (QTc > 500 ms).

Portable chest radiographs on 17 and 20 March 2020 showing progressive bilateral pulmonary infiltrates
Within 24 h following the tocilizumab infusion, there was an improvement in his fever, biomarkers ( Table 1 ) and hypoxaemia. Mechanical ventilation was avoided and he was monitored for another 6 day in the isolation unit. His saturations on room air improved to 90%. He was discharged home on 27 March, where he continued to make an uneventful recovery. Follow-up blood tests as an outpatient showed normalization of his lymphocyte count and CRP ( Table 1 ). His saturations on room air improved to 92%. A repeat nasopharyngeal and throat swab test for Covid-19 on 31 March was negative.
It has been postulated that there are three distinct but overlapping phases and pathological subsets of Covid-19 infection and subsequent Covid-19 disease in humans, the first two triggered by the virus itself and the third, by the host response.( 6 ) Treatment recommendations differ depending on the stage of the Covid-19 disease: the viral response phase (about 1–6 days after start of symptoms), the pneumonic phase (about days 6–10) which may progress to acute lung injury and ARDS, and the hyperinflammatory phase which typically occurs after day 8 in a minority of patients. This last phase is associated with worsening ARDS, multi-organ dysfunction syndrome (MODS), coagulation abnormalities, myocarditis and death. Patients progressing to this last severe phase of Covid-19 have clinical and laboratory evidence of an exaggerated inflammatory response, similar to the CRS, with persistent fever, worsening ARDS, elevated inflammatory markers and proinflammatory cytokines and MODS.
The Covid-19 virus binds to alveolar epithelial cells, activating the innate and adaptive immune systems resulting in the release of pro-inflammatory cytokines. This can lead to the CRS which is characterised by a hyperinflammatory state with raised inflammatory cytokines and biomarkers such as interleukin (IL)-2, IL-6, IL-7, granulocyte-colony stimulating factor, macrophage inflammatory protein 1-α, tumour necrosis factor-α, CRP, ferritin, Pro-BNP and D-dimer.( 7 ) The clinical picture is one of progressive ARDS and fulminant MODS.
Although corticosteroids are not routinely recommended for the treatment of Covid-19-associated lung injury, CRS immunosuppression with corticosteroids and other therapies is likely to be beneficial. Although there are currently no controlled clinical trials on the use of corticosteroids in Covid-19 patients, several published reports of corticosteroid therapy in severe Covid-19 have shown a shorter duration of supplemental oxygen use, improved radiographic findings and lower mortality in patients with ARDS.( 8 , 9 )
Tocilizumab, an IL-6 receptor blocker registered for CRS treatment, is being investigated for the treatment of patients with severe Covid-19, CRS and elevated IL-6 levels. IL-6 plays an important role in CRS and tocilizumab binds specifically to both soluble and membrane-bound IL-6 receptors (sIL-6R and mIL-6R), inhibiting sIL-6R and mIL-6R-mediated signalling. Small observational studies support the concept that tocilizumab may be an effective drug for patients with severe Covid-19 and respiratory failure requiring mechanical ventilation.( 10 , 11 ) In a study of 21 patients with Covid-19-related ARDS who received tocilizumab, the ICU mortality was less than 5%, all surviving patients became apyrexial within 72 h, pulmonary infiltrates on follow-up CT scan improved in 90%, hypoxaemia resolved in the majority and 90.5% of patients were discharged from the ICU after a median of 13.5 days.( 12 ) A large randomised, double-blind, placebo-controlled phase 3 clinical trial to evaluate the safety and efficacy of tocilizumab plus standard of care in hospitalised adult patients with severe Covid-19 pneumonia and ARDS has been being initiated.( 13 )
Currently, tocilizumab is available in South Africa for patients with severe Covid-19 and ARDS under the Monitored Emergency use of Unregistered and Investigational Interventions framework.( 14 ) This requires the treating physician to consult with an expert panel prior to enrolment, detailed patient data collection and ensuring that the patient meets the strict inclusion and exclusion criteria. Other immune modulating agents under investigation include siltuximab (IL-6 inhibitor), bevacizumab (vascular endothelial growth factor inhibitor), convalescent plasma from patients who have recovered from SARS-CoV-2 infection and intravenous immune globulin (Polygam).( 15 , 16 )
This case study also highlights some of the many controversies and complications in managing patients with severe Covid-19:
- • The use of inhaled or oral corticosteroids as a risk factor for severe Covid-19 is not certain. Individuals taking long-term corticosteroids for chronic conditions such as asthma, allergies and arthritis may be unable to mount an appropriate immune response and are generally considered high risk for severe disease if infected with Covid-19.( 17 ) Corticosteroids can also result in increased viral replication and prolonged viral shedding. Even a short course of oral corticosteroids in the preceding month for an asthma exacerbation, such as in this case study, is a risk factor for ARDS and mechanical ventilation.( 18 ) Conversely, in vitro studies with ciclesonide showed antiviral activity against Covid-19, and there have been reports of clinical effectiveness of inhaled ciclesonide in the treatment of Covid-19.( 19 ) Studies are currently underway to investigate whether inhaled ciclesonide alone, or in combination with hydroxychloroquine, could eradicate SARS-CoV-2 from respiratory tract earlier in patients with mild Covid-19.( 20 )
- • Diagnosis of SARS-CoV-2 pneumonia is not always straightforward. Currently, the gold standard in clinical practice is the detection of Covid-19 RNA by RT-PCR in respiratory tract specimens. Nasopharyngeal and throat swabs are recommended over expectorated or induced sputum. Lower respiratory tract specimens, such as tracheal aspirates or bronchoalveolar lavage in intubated patients may have higher viral loads and be more likely to yield positive tests (up to 95% sensitive) but come with a higher risk of transmission of infection to health-care workers.( 21 ) False-negative tests from upper respiratory specimens have been documented, as with this case study. If initial testing is negative in a patient with risk factors for infection and clinical or radiological features are highly suggestive of Covid-19 or determining the presence of infection is important for further management and infection control, repeat testing is recommended.
- • Chloroquine, azithromycin and lopinavir/ritonavir can all cause QT prolongation and ventricular arrhythmia, in particular drug-induced torsades de pointes and sudden cardiac death.( 22 ) Patients treated with any combination of these drugs should have 12–24 hourly ECG with QTc monitoring. If QTc >500 ms (as in the case study), or QTc increases >60 ms from baseline after initiating drug therapy, discontinue azithromycin and lopinavir/ritonavir, and consider reducing dose of chloroquine. Frequent monitoring of QTc is mandatory and chloroquine should also be discontinued if QTc remains >500 ms. The risk of serious ventricular arrhythmia may be reduced by performing a screening ECG prior to initiation of therapy, inquiring about a personal or family history of QT interval prolongation or sudden unexplained cardiac death, avoiding exposure to other medications known to affect QT interval, and aggressively treating hypocalcaemia, hypokalaemia and hypomagnesaemia. Hypokalaemia is especially common in patients with Covid-19 and is associated with a poorer prognosis.( 23 ) The correction of hypokalaemia can be challenging due to continuous renal loss of potassium resulting from the degradation of angiotensin converting enzyme 2 by binding of SAR-CoV-2.
This case study of severe Covid-19 pneumonia and CRS illustrates some of the diagnostic and therapeutic challenges and controversies regarding the management of this novel and complex infection. Meticulous monitoring for and early treatment of the hyperinflammatory phase of the disease may be crucial in preventing progression to severe ARDS, MODS and death.
ACKNOWLEDGEMENTS
We thank Dr L. Brannigan for his assistance with the management of this patient, and Dr E. Boschoff for the radiographs.
An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
- My Bibliography
- Collections
- Citation manager
Save citation to file
Email citation, add to collections.
- Create a new collection
- Add to an existing collection
Add to My Bibliography
Your saved search, create a file for external citation management software, your rss feed.
- Search in PubMed
- Search in NLM Catalog
- Add to Search
A case study of asthma care in school age children using nurse-coordinated multidisciplinary collaborative practices
Affiliations.
- 1 Faculty of Society and Health, Buckinghamshire New University, High Wycombe, UK.
- 2 Centre for Research in Primary and Community Care (CRIPACC), University of Hertfordshire, Hatfield, UK.
- 3 Centre for Health Services Studies, University of Kent, Canterbury, UK.
- PMID: 25914542
- PMCID: PMC4399592
- DOI: 10.2147/JMDH.S71030
Aim: To describe the role of school nursing in leading and coordinating a multidisciplinary networked system of support for children with asthma, and to analyze the strengths and challenges of undertaking and supporting multiagency interprofessional practice.
Background: The growth of networked and interprofessional collaborations arises from the recognition that a number of the most pressing public health problems cannot be addressed by single-discipline or -agency interventions. This paper identifies the potential of school nursing to provide the vision and multiagency leadership required to coordinate multidisciplinary collaboration.
Method: A mixed-method single-case study design using Yin's approach, including focus groups, interviews, and analysis of policy documents and public health reports.
Results: A model that explains the integrated population approach to managing school-age asthma is described; the role of the lead school nurse coordinator was seen as critical to the development and sustainability of the model.
Conclusion: School nurses can provide strategic multidisciplinary leadership to address pressing public health issues. Health service managers and commissioners need to understand how to support clinicians working across multiagency boundaries and to identify how to develop leadership skills for collaborative interprofessional practice so that the capacity for nursing and other health care professionals to address public health issues does not rely on individual motivation. In England, this will be of particular importance to the commissioning of public health services by local authorities from 2015.
Keywords: leadership; multiagency; public health; school nursing; whole systems.
PubMed Disclaimer
Similar articles
- Critical Care Network in the State of Qatar. Hijjeh M, Al Shaikh L, Alinier G, Selwood D, Malmstrom F, Hassan IF. Hijjeh M, et al. Qatar Med J. 2019 Nov 7;2019(2):2. doi: 10.5339/qmj.2019.qccc.2. eCollection 2019. Qatar Med J. 2019. PMID: 31763205 Free PMC article.
- Japan as the front-runner of super-aged societies: Perspectives from medicine and medical care in Japan. Arai H, Ouchi Y, Toba K, Endo T, Shimokado K, Tsubota K, Matsuo S, Mori H, Yumura W, Yokode M, Rakugi H, Ohshima S. Arai H, et al. Geriatr Gerontol Int. 2015 Jun;15(6):673-87. doi: 10.1111/ggi.12450. Epub 2015 Feb 5. Geriatr Gerontol Int. 2015. PMID: 25656311
- The Effectiveness of Integrated Care Pathways for Adults and Children in Health Care Settings: A Systematic Review. Allen D, Gillen E, Rixson L. Allen D, et al. JBI Libr Syst Rev. 2009;7(3):80-129. doi: 10.11124/01938924-200907030-00001. JBI Libr Syst Rev. 2009. PMID: 27820426
- Experiences of registered nurses as managers and leaders in residential aged care facilities: a systematic review. Dwyer D. Dwyer D. Int J Evid Based Healthc. 2011 Dec;9(4):388-402. doi: 10.1111/j.1744-1609.2011.00239.x. Int J Evid Based Healthc. 2011. PMID: 22093388 Review.
- Educational interventions to enhance competencies for interprofessional collaboration among nurse and physician managers: An integrative review. Clausen C, Cummins K, Dionne K. Clausen C, et al. J Interprof Care. 2017 Nov;31(6):685-695. doi: 10.1080/13561820.2017.1347153. Epub 2017 Sep 1. J Interprof Care. 2017. PMID: 28862885 Review.
- A model to facilitate collaborative social support for pregnant students in secondary schools. Matlala SF. Matlala SF. J Multidiscip Healthc. 2017 Sep 28;10:383-389. doi: 10.2147/JMDH.S142139. eCollection 2017. J Multidiscip Healthc. 2017. PMID: 29026315 Free PMC article.
- Kendall S, Wilson P, Procter S, Brooks F, Bunn F, McNeilly E. The Nursing Contribution to Models of Chronic Disease Management. Report to NIHR Service Delivery and Organisation Programme. England: 2010. [Accessed August 4, 2014]. Available from: http://www.netscc.ac.uk/hsdr/files/project/SDO_FR_08-1605-121_V01.pdf .
- Procter S, Wilson PM, Brooks F, Kendall S. Success and failure in integrated models of nursing for long term conditions: multiple case studies of whole systems. Int J Nurs Stud. 2013;50(5):632–643. - PubMed
- World Health Organisation . Primary Health Care Now More than Ever. Geneva: WHO; 2008.
- Royal college of physicians . The National Review of Asthma Deaths. Royal college of Physicians; London: 2014. Why asthma still kills.
- Julious SA, Osman LM, Jiwa M. Increases in asthma hospital admissions associated with the end of summer vacation for school-age children with asthma in two cities from England and Scotland. Public Health. 2007;121(6):482–484. - PubMed
LinkOut - more resources
Full text sources.
- Dove Medical Press
- Europe PubMed Central
- PubMed Central

- Citation Manager
NCBI Literature Resources
MeSH PMC Bookshelf Disclaimer
The PubMed wordmark and PubMed logo are registered trademarks of the U.S. Department of Health and Human Services (HHS). Unauthorized use of these marks is strictly prohibited.
- Campus Directory
- Current Students
- Faculty & Staff

Asthma Case Study
Asthma affects about 6.1 million children in the US under 18 years of age, making it one of the most common chronic childhood disorders (American Lung Association, 2021). Asthma occurs as a result of a stimulus which can range from allergens, cigarette smoke, changes in temperature, stress, or exercise. In this case we’ll experience an asthma attack and subsequent treatment with 16-year-old Ben Mason.
Module 9: Asthma

Review structure and functions of the respiratory system...
Asthma - Page 1

Ben was struggling to breathe when he reached the ER...
Asthma - Page 2
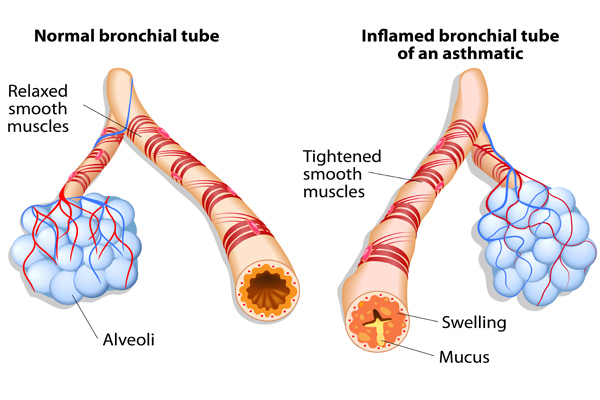
Ben was also given an additional breathing treatment...
Asthma - Page 3
Case Summary
Summary of the Case
Asthma - Summary

Answers to Case Questions
Asthma - Answers

Professionals
Health Professionals Introduced in Case
Asthma - Professionals
Additional Links
Asthma - Links
- Search Menu
- Sign in through your institution
- Advance Articles
- Supplements
- Author Guidelines
- Reviewer guidelines
- Submission Site
- Open Access
- Self-Archiving Policy
- Why Publish?
- Advertising & Corporate Services
- Advertising
- Reprints and ePrints
- Sponsored Supplements
- Branded Books
- Journals Career Network
- About Paediatrics & Child Health
- About The Canadian Paediatric Society
- Editorial Board
- Journals on Oxford Academic
- Books on Oxford Academic

Article Contents
Case 1 diagnosis: allergy bullying, clinical pearls.
- < Previous
Case 1: A 12-year-old girl with food allergies and an acute asthma exacerbation
- Article contents
- Figures & tables
- Supplementary Data
Lopamudra Das, Michelle GK Ward, Case 1: A 12-year-old girl with food allergies and an acute asthma exacerbation, Paediatrics & Child Health , Volume 19, Issue 2, February 2014, Pages 69–70, https://doi.org/10.1093/pch/19.2.69
- Permissions Icon Permissions
A 12-year-old girl with a history of asthma presented to the emergency department with a three-day history of increased work of breathing, cough and wheezing. She reported no clear trigger for her respiratory symptoms, although she had noted some symptoms of a mild upper respiratory tract infection. With this episode, the patient had been using a short-acting bronchodilator more frequently than she had in the past, without the expected resolution of symptoms.
On the day of presentation, the patient awoke feeling ‘suffocated’ and her mother noted her lips to be blue. In the emergency department, her oxygen saturation was 85% and her respiratory rate was 40 breaths/min. She had significantly increased work of breathing and poor air entry bilaterally to both lung bases, with wheezing in the upper lung zones. She was treated with salbutamol/ipratropium and received intravenous steroids and magnesium sulfate. Her chest x-ray showed hyperinflation and no focal findings.
Her medical history revealed that she was followed by a respirologist for her asthma, had good medication adherence and had not experienced a significant exacerbation for six months. She also had a history of wheezing, dyspnea and pruritis with exposure to peanuts, chickpeas and lentils; she had been prescribed an injectible epinephrine device for this. However, her device had expired at the time of presentation. In the past, her wheezing episodes had been seasonal and related to exposure to grass and pollens; this presentation occurred during the winter. Further history revealed the probable cause of her presentation.
Although reluctant to disclose the information, our patient later revealed that she had been experiencing significant bullying at school, which was primarily related to her food allergies. Three days before her admission, classmates had smeared peanut butter on one of her schoolbooks. She developed pruritis immediately after opening the book and she started wheezing and coughing later that day. This event followed several months of being taunted with peanut products at school. The patient was experiencing low mood and reported new symptoms of anxiety related to school. The review of systems was otherwise negative, with no substance use.
The patient's asthma exacerbation resolved with conventional asthma treatment. Her pulmonary function tests were nonconcerning (forced expiratory volume in 1 s 94% and 99% of predicted) after her recovery. The trigger for her asthma exacerbation was likely multifactorial, related to exposure to the food allergen as well as the upper respiratory infection. A psychologist was consulted to assess the symptoms of anxiety and depression that had occurred as a result of the bullying. During the hospitalization, the medical team contacted the patient's school to provide education on allergy bullying, treatment of severe allergic reactions and its potential for life-threatening reactions with exposure to allergens. The medical team also recommended community resources for further education of students and staff about allergy bullying and its prevention.
Allergy bullying is a form of bullying with potentially severe medical outcomes. In recent years, it has gained increasing notoriety in schools and in the media. Population-based studies have shown that 20% to 35% of children with allergies experience bullying. In many cases (31% in one recent study [ 1 ]), this bullying is related directly to the food allergy. From a medical perspective, there are little published data regarding allergy bullying, and many health care providers may not be aware of the issue.
Allergy bullying can include teasing a child about their allergy, throwing food at a child, or even forcing them to touch or eat allergenic foods. Most episodes of allergy bullying occur at school, and can include episodes perpetrated by teachers and/or staff ( 2 ).
Allergy bullying can lead to allergic reactions, which may be mild or severe (eg, urticaria, wheezing, anaphylaxis), but may also lead to negative emotional consequences (sadness, depression) ( 2 ) and an overall decrease in quality of life measures ( 1 ). Adolescents commonly resist using medical devices, such as injectible epinephrine devices, and bullying may be a contributing factor for this ( 3 ). Attempting to conceal symptoms in a bullying situation may place children at risk for a worse outcome.
Physicians can play a key role in detecting allergy bullying and its health consequences. In many cases, children have not discussed this issue with their parents ( 1 ). Given the prevalence of bullying, its potential to lead to severe harm, including death, and the lack of awareness of this issue, clinicians should specifically ask about bullying in all children and teens with allergies. Physicians can also work with families and schools to support these children, educate their peers and school staff, and help prevent negative health outcomes from allergy bullying.
Online resources
www.anaphylaxis.ca − A national charity that aims to inform, support, educate and advocate for the needs of individuals and families living with anaphylaxis, and to support and participate in research. This website includes education modules for schools and links to local support groups throughout Canada.
www.whyriskit.ca/pages/en/live/bullying.php − A website for teenagers with food allergies; includes a segment that addresses food bullying.
www.foodallergy.org − Contains numerous resources for children and their families, including a significant discussion on bullying and ways to prevent it.
Allergy bullying is common but is often unrecognized as a factor in clinical presentations of allergic reactions.
Physicians should make a point of asking about bullying in patients with allergies and become familiar with resources for dealing with allergy bullying.
Physicians can play roles as advocates, educators and collaborators with the school system to help make the school environment safer for children with allergies who may be at risk for allergy bullying.
Google Scholar
| Month: | Total Views: |
|---|---|
| February 2017 | 2 |
| June 2017 | 2 |
| November 2017 | 3 |
| December 2017 | 6 |
| January 2018 | 3 |
| February 2018 | 5 |
| March 2018 | 7 |
| April 2018 | 10 |
| May 2018 | 8 |
| June 2018 | 13 |
| July 2018 | 3 |
| August 2018 | 5 |
| September 2018 | 8 |
| October 2018 | 6 |
| November 2018 | 8 |
| December 2018 | 22 |
| January 2019 | 1 |
| February 2019 | 8 |
| March 2019 | 3 |
| April 2019 | 13 |
| May 2019 | 9 |
| June 2019 | 5 |
| July 2019 | 17 |
| August 2019 | 12 |
| September 2019 | 15 |
| October 2019 | 6 |
| November 2019 | 3 |
| December 2019 | 4 |
| January 2020 | 8 |
| February 2020 | 10 |
| March 2020 | 16 |
| April 2020 | 44 |
| May 2020 | 65 |
| June 2020 | 102 |
| July 2020 | 119 |
| August 2020 | 104 |
| September 2020 | 221 |
| October 2020 | 286 |
| November 2020 | 391 |
| December 2020 | 336 |
| January 2021 | 456 |
| February 2021 | 492 |
| March 2021 | 661 |
| April 2021 | 646 |
| May 2021 | 662 |
| June 2021 | 507 |
| July 2021 | 389 |
| August 2021 | 484 |
| September 2021 | 628 |
| October 2021 | 860 |
| November 2021 | 752 |
| December 2021 | 627 |
| January 2022 | 599 |
| February 2022 | 698 |
| March 2022 | 922 |
| April 2022 | 913 |
| May 2022 | 728 |
| June 2022 | 450 |
| July 2022 | 299 |
| August 2022 | 406 |
| September 2022 | 668 |
| October 2022 | 956 |
| November 2022 | 915 |
| December 2022 | 771 |
| January 2023 | 649 |
| February 2023 | 707 |
| March 2023 | 769 |
| April 2023 | 646 |
| May 2023 | 748 |
| June 2023 | 428 |
| July 2023 | 356 |
| August 2023 | 387 |
| September 2023 | 567 |
| October 2023 | 743 |
| November 2023 | 691 |
| December 2023 | 524 |
| January 2024 | 493 |
| February 2024 | 667 |
| March 2024 | 743 |
| April 2024 | 767 |
| May 2024 | 750 |
| June 2024 | 333 |
| July 2024 | 283 |
| August 2024 | 335 |
Email alerts
Citing articles via, looking for your next opportunity.
- About Paediatrics & Child Health
- Recommend to Your Librarian
- Advertising and Corporate Services
Affiliations
- Online ISSN 1918-1485
- Print ISSN 1205-7088
- Copyright © 2024 Oxford University Press
- About Oxford Academic
- Publish journals with us
- University press partners
- What we publish
- New features
- Open access
- Institutional account management
- Rights and permissions
- Get help with access
- Accessibility
- Media enquiries
- Oxford University Press
- Oxford Languages
- University of Oxford
Oxford University Press is a department of the University of Oxford. It furthers the University's objective of excellence in research, scholarship, and education by publishing worldwide
- Copyright © 2024 Oxford University Press
- Cookie settings
- Cookie policy
- Privacy policy
- Legal notice
This Feature Is Available To Subscribers Only
Sign In or Create an Account
This PDF is available to Subscribers Only
For full access to this pdf, sign in to an existing account, or purchase an annual subscription.
A case study of asthma care in school age children using nurse-coordinated multidisciplinary collaborative practices
- CC BY-NC 3.0

- Buckinghamshire New University

- University of Technology Sydney

- University of Kent

Discover the world's research
- 25+ million members
- 160+ million publication pages
- 2.3+ billion citations
- Solange Meira de Sousa

- Expet Rev Clin Immunol

- Maki KARIYAZAKI
- Satoko Tsuru
- Takanori MOTOKI
- Masako Fujiwara

- Rita Araujo
- Janeke Zoetmann

- Ariel Plante
- Abigail Zavod
- Sarah C. Akerman
- Martha M. Snow

- Lect Notes Comput Sci

- Prim Health Care Res Dev
- BMC HEALTH SERV RES

- J PUBL ADM RES THEOR

- IMPLEMENT SCI
- Roman Kislov
- Kieran Walshe

- Recruit researchers
- Join for free
- Login Email Tip: Most researchers use their institutional email address as their ResearchGate login Password Forgot password? Keep me logged in Log in or Continue with Google Welcome back! Please log in. Email · Hint Tip: Most researchers use their institutional email address as their ResearchGate login Password Forgot password? Keep me logged in Log in or Continue with Google No account? Sign up
- Join our Mailing List
Working locally in primary care and collaborating globally to improve respiratory health
Clinical case study - asthma, clinical case study - asthma, resource information.
- Disease management
That's incorrect. His FEV is 50% of normal, which indicates that he is in the severe range. Also he has needed his rescue inhaler every day. He may not stay at this level with step up treatment. His classification may be changed if his symptoms move to a lower level . Click the continue button below to move on . No, his FEV is 50% of normal, which indicates that he is in the severe range. Also he has needed his rescue inhaler every day. He may not stay at this level with step up treatment. His classification may be changed if his symptoms move to a lower level. Click the continue button below to move on . Asthma as a risk factor and allergic rhinitis as a protective factor for COVID-19 severity: a case-control study
Cite this article
The COVID-19 pandemic has resulted in significant global morbidity and mortality. The disease presents a broad clinical spectrum, significantly influenced by underlying comorbidities. While certain conditions are known to exacerbate COVID-19 outcomes, the role of chronic inflammatory airway diseases such as asthma and rhinitis in influencing disease severity remains controversial. This study investigates the association between asthma and allergic rhinitis and the severity of COVID-19 outcomes in a specific geographical region prior to widespread vaccine deployment. We conducted a case-control study with unvaccinated adult patients who had laboratory-confirmed COVID-19 by polymerase chain reaction (PCR). Cases were defined as severe or critical COVID-19 patients requiring intensive care unit (ICU) admission, and controls were non-severe patients without signs of viral pneumonia or hypoxia. We utilized the International Study of Asthma and Allergies in Childhood (ISAAC) questionnaire to assess the presence of asthma and allergic rhinitis. The association between these chronic inflammatory airway diseases and the severity of COVID-19 was evaluated using multivariate logistic regression analysis. A total of 122 patients were analyzed, with 61 in each group. The presence of asthma (9 patients) was associated with an increased likelihood of severe COVID-19 (OR = 13.0; 95% CI 1.27-133.74), while rhinitis (39 patients) was associated with a protective effect against severe outcomes (OR = 0.36; 95% CI 0.13–0.99). No significant association was found between the frequency of asthmatic episodes or the severity of rhinitis and the severity of COVID-19 outcomes. This study underscores the divergent effects of chronic inflammatory airway diseases on COVID-19 severity, with asthma associated with a higher likelihood of severe outcomes and rhinitis potentially offering protective effects. These findings enhance our understanding of the complex interactions between respiratory allergies and COVID-19, emphasizing the importance of targeted clinical management and public health strategies. Key message• Asthma increases the likelihood of severe COVID-19 outcomes. • Allergic rhinitis may provide protection against severe COVID-19. • Comorbidities strongly influence COVID-19 severity. This is a preview of subscription content, log in via an institution to check access. Access this articleSubscribe and save.
Price includes VAT (Russian Federation) Instant access to the full article PDF. Rent this article via DeepDyve Institutional subscriptions  Similar content being viewed by others Prognosis of COVID-19 in respiratory allergy: a systematic review and meta-analysis How does allergic rhinitis impact the severity of COVID-19?: a case–control study The association between COVID-19 vaccine/infection and new-onset asthma in children - based on the global TriNetX databaseData availability. The data supporting this study’s findings are available from the corresponding author, upon reasonable request. Yang JM, Koh HY, Moon SY et al (2020) Allergic disorders and susceptibility to and severity of COVID-19: a nationwide cohort study. J Allergy Clin Immunol 146:790–798. https://doi.org/10.1016/j.jaci.2020.08.008 Article CAS PubMed PubMed Central Google Scholar Gao Y, Ding M, Dong X et al (2021) Risk factors for severe and critically ill COVID-19 patients: a review. Allergy 76:428–455. https://doi.org/10.1111/all.14657 Article CAS PubMed Google Scholar Gasmi A, Peana M, Pivina L et al (2021) Interrelations between COVID-19 and other disorders. Clin Immunol 224:108651. https://doi.org/10.1016/j.clim.2020.108651 Martins-Filho PR, Araújo AAS, Góes MAO et al (2021) COVID-19 mortality and case-fatality rates in Sergipe State, Northeast Brazil, from April to June 2020. Front Public Heal 9:581618. https://doi.org/10.3389/fpubh.2021.581618 Article Google Scholar Martins-Filho PR, Antunes de Souza Araújo A, Pereira LX et al (2021) Factors Associated with mortality among hospitalized patients with COVID-19: a retrospective cohort study. Am J Trop Med Hyg 104:103–105. https://doi.org/10.4269/ajtmh.20-1170 Zhang J, Dong X, Liu G, Gao Y (2022) Risk and protective factors for COVID-19 morbidity, severity, and Mortality. Clin Rev Allergy Immunol 64:90–107. https://doi.org/10.1007/s12016-022-08921-5 Guvey A (2021) How does allergic rhinitis impact the severity of COVID-19? A case–control study. Eur Arch Oto-Rhino-Laryngology 278:4367–4371. https://doi.org/10.1007/s00405-021-06836-z Shi W, Gao Z, Ding Y et al (2020) Clinical characteristics of COVID-19 patients combined with allergy. Allergy 75:2405–2408. https://doi.org/10.1111/all.14434 Jiao L, Bujnowski D, Liu P et al (2024) Asthma and clinical outcomes of COVID-19 in a community setting. Public Health 226:84–90. https://doi.org/10.1016/j.puhe.2023.10.040 Zhu Z, Hasegawa K, Ma B et al (2020) Association of Asthma and its genetic predisposition with the risk of severe COVID-19. J Allergy Clin Immunol 146:327–329e4. https://doi.org/10.1016/j.jaci.2020.06.001 Wang Y, Ao G, Qi X, Xie B (2020) The association between COVID-19 and asthma: a systematic review and meta‐analysis. Clin Exp Allergy 50:1274–1277. https://doi.org/10.1111/cea.13733 Kimura H, Francisco D, Conway M et al (2020) Type 2 inflammation modulates ACE2 and TMPRSS2 in airway epithelial cells. J Allergy Clin Immunol 146:80–88e8. https://doi.org/10.1016/j.jaci.2020.05.004 Yao Y, Wang H, Liu Z (2020) Expression of ACE2 in airways: implication for COVID-19 risk and disease management in patients with chronic inflammatory respiratory diseases. Clin Exp Allergy 50:1313–1324. https://doi.org/10.1111/cea.13746 von Elm E, Altman DG, Egger M et al (2007) The strengthening the reporting of Observational studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet 370:1453–1457 Martins-Filho PR, de Souza Araújo AA, Quintans-Júnior LJ et al (2022) Dynamics of hospitalizations and in-hospital deaths from COVID-19 in northeast Brazil: a retrospective analysis based on the circulation of SARS-CoV-2 variants and vaccination coverage. Epidemiol Health 44:e2022036. https://doi.org/10.4178/epih.e2022036 Marshall JC, Murthy S, Diaz J et al (2020) A minimal common outcome measure set for COVID-19 clinical research. Lancet Infect Dis 20:e192–e197. https://doi.org/10.1016/S1473-3099(20)30483-7 Article CAS Google Scholar Asher M, Keil U, Anderson H et al (1995) International Study of Asthma and allergies in Childhood (ISAAC): rationale and methods. Eur Respir J 8:483–491. https://doi.org/10.1183/09031936.95.08030483 Solé D, Vanna AT, Yamada E et al (1998) International Study of Asthma and allergies in Childhood (ISAAC) written questionnaire: validation of the asthma component among Brazilian children. J Investig Allergol Clin Immunol 8:376–382 PubMed Google Scholar Solé D, Wandalsen GF, Camelo-Nunes IC et al (2006) Prevalence of symptoms of asthma, rhinitis, and atopic eczema among Brazilian children and adolescents identified by the International Study of Asthma and allergies in Childhood (ISAAC) - phase 3. J Pediatr (Rio J) 82:341–346. https://doi.org/10.2223/JPED.1521 Article PubMed Google Scholar Oliveira TB, Persigo ALK, Ferrazza CC et al (2020) Prevalence of asthma, allergic rhinitis and pollinosis in a city of Brazil: a monitoring study. Allergol Immunopathol (Madr) 48:537–544. https://doi.org/10.1016/j.aller.2020.03.010 Urrutia-Pereira M, Chong-Neto H, Mocellin LP et al (2021) Prevalence of asthma symptoms and associated factors in adolescents and adults in southern Brazil: A Global Asthma Network Phase I study. World Allergy Organ J 14:100529. https://doi.org/10.1016/j.waojou.2021.100529 Article PubMed PubMed Central Google Scholar Barbarot S, Auziere S, Gadkari A et al (2018) Epidemiology of atopic dermatitis in adults: results from an international survey. Allergy 73:1284–1293. https://doi.org/10.1111/all.13401 Peñaranda A, Pérez-Herrera LC, Gantiva M et al (2023) Factors associated with allergic rhinitis and combined allergic rhinitis and asthma syndrome (CARAS) in adults undergoing immunotherapy in a tropical country: is ISAAC-III questionnaire useful in adult populations? Allergol Immunopathol (Madr) 51:78–86. https://doi.org/10.15586/aei.v51i4.833 Hoffmann M, Kleine-Weber H, Schroeder S et al (2020) SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell 181:271–280e8. https://doi.org/10.1016/j.cell.2020.02.052 Matsumoto K, Saito H (2020) Does asthma affect morbidity or severity of COVID-19? J Allergy Clin Immunol 146:55–57. https://doi.org/10.1016/j.jaci.2020.05.017 Ren J, Pang W, Luo Y et al (2022) Impact of allergic Rhinitis and Asthma on COVID-19 infection, hospitalization, and Mortality. J Allergy Clin Immunol Pract 10:124–133. https://doi.org/10.1016/j.jaip.2021.10.049 Ziegler CGK, Allon SJ, Nyquist SK et al (2020) SARS-CoV-2 receptor ACE2 is an Interferon-stimulated gene in human airway epithelial cells and is detected in specific cell subsets across tissues. Cell 181:1016–1035e19. https://doi.org/10.1016/j.cell.2020.04.035 Grifoni A, Weiskopf D, Ramirez SI et al (2020) Targets of T cell responses to SARS-CoV-2 coronavirus in humans with COVID-19 disease and unexposed individuals. Cell 181:1489–1501e15. https://doi.org/10.1016/j.cell.2020.05.015 Skevaki C, Karsonova A, Karaulov A et al (2020) Asthma-associated risk for COVID-19 development. J Allergy Clin Immunol 146:1295–1301. https://doi.org/10.1016/j.jaci.2020.09.017 Samitas K, Carter A, Kariyawasam HH, Xanthou G (2018) Upper and lower airway remodelling mechanisms in asthma, allergic rhinitis and chronic rhinosinusitis: the one airway concept revisited. Allergy 73:993–1002. https://doi.org/10.1111/all.13373 Chen C, Song X, Murdock DJ et al (2024) Association between allergic conditions and COVID-19 susceptibility and outcomes. Ann Allergy Asthma Immunol 132:637–645e7. https://doi.org/10.1016/j.anai.2024.01.011 Valle SOR, Kuschnir FC, Solé D et al (2012) Validity and reproducibility of the Asthma Core International Study of Asthma and allergies in Childhood (ISAAC) Written Questionnaire obtained by Telephone Survey. J Asthma 49:390–394. https://doi.org/10.3109/02770903.2012.669440 Download references AcknowledgementsPRMF is a research productivity fellow at the National Council for Scientific and Technological Development (CNPq), Brazil. This study did not receive financial support. Author informationAuthors and affiliations. Graduate Program in Health Sciences, Federal University of Sergipe, Aracaju, SE, Brazil Martha Débora Lira Tenório, Roque Pacheco de Almeida, Amélia Ribeiro de Jesus & Paulo Ricardo Martins-Filho Investigative Pathology Laboratory, Federal University of Sergipe, Aracaju, SE, Brazil Martha Débora Lira Tenório & Paulo Ricardo Martins-Filho Department of Medicine, Federal University of Sergipe, Aracaju, SE, Brazil Gabriel Valentim dos Santos Menezes Siqueira, Gustavo Costa Caldas, Roque Pacheco de Almeida & Amélia Ribeiro de Jesus Hospital Universitário, Laboratório de Patologia Investigativa, Universidade Federal de Sergipe, Rua Cláudio Batista, s/n. Sanatório, Aracaju, CEP: 49060-100, Sergipe, Brasil Paulo Ricardo Martins-Filho You can also search for this author in PubMed Google Scholar ContributionsMDLT contributed to the conception, study design, data collection, data analysis, interpretation, writing of the manuscript, and manuscript revisions. GVSMS and GCC contributed to the data collection, interpretation, and manuscript revisions. RPA and ARJ contributed to the conception, study design, interpretation, and manuscript revisions. PRMF contributed to the study design, data collection, data analysis, interpretation, writing of the manuscript, and manuscript revisions. All authors have read and agreed to the published version of the manuscript. Corresponding authorCorrespondence to Paulo Ricardo Martins-Filho . Ethics declarationsConflict of interest. The authors have no conflict of interest to declare. Additional informationPublisher’s note. Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations. Electronic supplementary materialBelow is the link to the electronic supplementary material. Supplementary Material 1Rights and permissions. Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law. Reprints and permissions About this articleLira Tenório, M., dos Santos Menezes Siqueira, G., Costa Caldas, G. et al. Asthma as a risk factor and allergic rhinitis as a protective factor for COVID-19 severity: a case-control study. Eur Arch Otorhinolaryngol (2024). https://doi.org/10.1007/s00405-024-08893-6 Download citation Received : 27 May 2024 Accepted : 03 August 2024 Published : 24 August 2024 DOI : https://doi.org/10.1007/s00405-024-08893-6 Share this articleAnyone you share the following link with will be able to read this content: Sorry, a shareable link is not currently available for this article. Provided by the Springer Nature SharedIt content-sharing initiative
Official websites use .gov A .gov website belongs to an official government organization in the United States. Secure .gov websites use HTTPS A lock ( ) or https:// means you've safely connected to the .gov website. Share sensitive information only on official, secure websites. Implementation and Evaluation of a School Nurse Toolkit to Reinforce Best Practices for Asthma Care in SchoolsPROGRAM EVALUATION BRIEF — Volume 21 — August 22, 2024 Diane Wing, MS 1 ; Evilia Jankowski, MSA, BSN, NCSN 2 ; John Dowling, MA 3 ; Tisa Vorce, MA, RRT 3 ( View author affiliations )Suggested citation for this article: Wing D, Jankowski E, Dowling J, Vorce T. Implementation and Evaluation of a School Nurse Toolkit to Reinforce Best Practices for Asthma Care in Schools. Prev Chronic Dis 2024;21:240027. DOI: http://dx.doi.org/10.5888/pcd21.240027 . PEER REVIEWED IntroductionPurpose and objectives, intervention approach, evaluation approach, implications for public health, acknowledgments, author information. What is already known on this topic? Resources reinforcing the standards of care for asthma can strengthen self-efficacy and use of asthma management practices among school nurses. What is added by this report? An asthma toolkit was promoted to school nurses in Michigan. School nurses viewed the toolkit and reported implementing changes to improve asthma management practices in their schools. What are the implications for public health practice? Reaching school nurses through promotional activities can encourage school nurses to apply the standards for care to support students with asthma in school. A toolkit, developed by a multidisciplinary team of national and statewide professionals, was promoted among school nurses in Michigan to support use of the standards of care for asthma in schools. We evaluated the effectiveness of the toolkit to assist school nurses in providing support for students with asthma. We used a multimethod approach to assess use of the toolkit, changes in nursing practices as a result of using the toolkit, and challenges encountered when implementing the standards for asthma care. During a 12-month period, from July 2022 through June 2023, increases in time on web page and monthly page views aligned with efforts to promote toolkit use. School nurses reported using the toolkit and implementing practice changes pertaining to training and education, ensuring proper use of and access to asthma medications, and advocating for self-carry of asthma medications. Challenges to implementing the standards of asthma care were time, parental engagement, institutional support, and identifying students with asthma. We found that our promotional efforts prompted school nurses to access the toolkit, which helped school nurses to effectuate practice changes to improve support for students with asthma in schools. The prevalence of current asthma in Michigan among children and adolescents aged 5 to 17 years is 8.8% (1). Of these children and adolescents, 35.3% missed 1 or more days of school due to asthma from 2017 to 2021 (2). Children and adolescents who are Black or in low-income households are disproportionately affected by asthma (2). From 2017 to 2021, 18.4% of Michigan children and adolescents aged 5 to 17 years with current asthma had an asthma-related visit to an emergency department or urgent care in the past 12 months; however, 30.9% of Black children and adolescents and 26.0% of children and adolescents in households with less than $50,000 in annual income had an asthma-related emergency department or urgent care visit in the past 12 months (2). Complex interactions among varying levels of social, structural, biological, and behavioral determinants contribute to asthma-related disparities (3). In June 2022, the Michigan State Board of Education updated a model policy for supporting students with asthma that set forth recommendations for schools to establish asthma-friendly environments to improve students’ attendance and participation in activities and promote academic success and well-being (4). Building on the Whole School, Whole Community, Whole Child model (5), which provides conceptual support and practical guidance central to best practices, the policy designated school nurses as important members of a child’s support network to coordinate asthma management activities; integrate communication among students, caregivers, and health care providers; and ensure all school personnel have received appropriate training in asthma management and emergency response (4,5). School nurses fill the gap between health care and education, provide both acute and chronic care, treat and assess behavioral health concerns, and connect students and families to community resources (6). Although school nurses are well positioned in their role to support students with asthma, inadequate time to devote to asthma management, due in part to competing student needs and multiple roles, impedes completion of these activities (7). Additionally, school nurses in Michigan practice in various models, and they may be responsible for covering more than 1 building or an entire school district. As such, a medically qualified person may not always be available to meet the emergent needs of students, and the oversight is shifted to school staff, teachers, and administrators (7). Historically, Michigan has ranked lowest among states in its school nurse-to-student ratio (8). However, due in part to recent increases in school budgets (9), the number of employed school nurses has quadrupled since 2019, increasing from some 200 nurses to an estimated 800 nurses (Evilia Jankowski, MSA, BSN, NCSN, State School Nurse Consultant, Michigan Department of Education, October 5, 2023, email correspondence). Younger and less experienced school nurses have been reported to be less likely than older and more experienced school nurses to perform asthma management activities (10). Regardless of experience, however, asthma-focused education can strengthen self-confidence in asthma management among school nurses (10,11), and this self-confidence has been associated with increased performance of asthma management activities (10). To support school nurses’ use of best practices for asthma management, a multidisciplinary team of national and statewide professionals convened to develop an asthma toolkit (12). The toolkit, Supporting Students with Asthma at School: Standards of Care, presents information for understanding asthma and applicable laws and details performance standards to support students with asthma (12). These standards include coordination of care, assembling health care plans, and training school personnel. The conceptualization of this evaluation was a collaborative effort between the Michigan Department of Education (MDE) and the Michigan Department of Health and Human Services (MDHHS) Asthma Prevention and Control Program. We designed the evaluation to assess the effectiveness of the toolkit to assist school nurses in providing support for students with asthma in schools. Our evaluation questions were 1) To what extent did school nurses use the toolkit? 2) What practice changes were implemented as a result of using the toolkit? and 3) What were the perceived challenges to implementing standards for asthma care in schools? On August 4, 2022, the toolkit was uploaded to the School Health Services page on the MDE website (12). The Michigan State School Nurse Consultant (SSNC) (E.J.) promoted the toolkit throughout the 2022–2023 school year. The SSNC introduced the toolkit at the Michigan School Nurse Summer Institute meeting in August 2022. The toolkit was promoted in the SSNC’s newsletter sent to school nurses in January 2023, during the SSNC’s monthly office hours in March 2023, and at the Michigan Association of School Nurses annual conference in May 2023. The MDHHS institutional review board determined the evaluation to be exempt from full review and oversight. We used a multimethod approach, which consisted of collecting quantitative and qualitative data from several sources to facilitate a complete understanding of the extent to which the toolkit was used. We used Google analytics to track the extent to which the home page of the toolkit was accessed from July 2022 through June 2023 on the MDE web page. The home page of the toolkit includes links to various components of the toolkit and a link to access and download a complete version of the toolkit document. We tracked time on page in seconds; the number of page views, defined as the number of times a web page was seen by all users; and the number of unique page views, defined as the average number of times a web page was seen by each user. School nurses were invited to complete an online survey, administered by SurveyMonkey (www.surveymonkey.com), once in January 2023 and again in February 2023. We used the SSNC’s newsletter to invite the 800 school nurse subscribers to complete the survey. Two survey questions were used to assess toolkit use and practice changes made. The first question was, “Have you used the Asthma Toolkit to help guide you on asthma care and management for students in school?” Response options were yes and no. The second question was open-ended: “Based on your use of the Asthma Toolkit, have you made any process or practice changes in the way students with asthma are supported? If yes, briefly describe the changes made.” In May 2023, the SSNC led a Kahoot! (www.kahoot.com) among school nurses attending the Michigan Association of School Nurses annual conference. A Kahoot! is a game-based platform used to collect real-time information from a group of people through a web browser on a mobile device. During the Kahoot!, 3 statements were used to collect information. The first was a true-or-false statement: “I have utilized the Asthma Toolkit on the MDE website.” The second was open-ended: “Share one practice change implemented since accessing the Asthma Toolkit.” The third was also open-ended: “What is the biggest challenge to implementing the standards of care for supporting students with asthma in school?” Responses to open-ended questions were limited to 250 characters. We used Microsoft Excel to conduct a descriptive analysis of count data. We calculated frequencies and means for time on page, number of page views and unique page views, and we calculated frequencies for the number of respondents who used the toolkit. For qualitative analysis, we identified and developed themes on the basis of respondents’ comments, and we created and condensed categories on the basis of commonalities among the themes. We used Microsoft Excel to assign comments to a column and themes to a row to track when a theme was mentioned. One person (D.W.) coded the information and developed the coding scheme, which was reviewed and discussed with 3 team members (E.J., J.D., T.V.). Comments from the survey and Kahoot! were analyzed and reported separately. Time on page totaled 6,124 seconds (1 hour, 42 minutes) and averaged 510 seconds (8 minutes, 30 seconds) per month. The least amount of time on page was 87 seconds in July 2022, the month before the toolkit was uploaded, and the greatest time on page was 1,049 seconds (17 minutes, 29 seconds) in March 2023. Page views totaled 819, averaged 68 per month, and ranged from 38 to 150. Unique page views totaled 648, averaged 54 per month, and ranged from 7 to 125. August and September had the greatest number of page views, and increases in page views generally aligned with efforts to promote toolkit use. The frequency of unique page views followed a similar pattern ( Figure ) . Of the 800 school nurses who subscribed to the SSNC’s newsletter, 71 completed a survey (9% response). Of the 71 respondents, 42 (59%) indicated they used the toolkit, and of these, 11 (26%) provided information on practice changes made. We identified 2 themes based on comments: training and education and asthma action plans. Respondents reported using the information to educate administrators, staff, and families, using resources from the toolkit for training, and improving their own skills in recording asthma episodes. They also reported implementing the use of standardized asthma action plans and requesting and obtaining asthma action plans for each student with asthma. Of the 176 meeting attendees, 140 participated in the Kahoot! (80% response). Of the 140 participants, 97 (69%) indicated that they used the toolkit, and of these, 73 (75%) provided information on practice changes as a result of toolkit use. Of these responses, 5 themes emerged: training and education (n = 25 respondents who made comments that pertained to a theme); asthma action plans or care plans (n = 19); use of asthma medications and spacers (n = 16); self-carry of asthma medications (n = 7); and other responses (n = 6). School nurses reported using the guidance to train staff, some specifically referencing the tier-level training and infographic resources in the toolkit; educate staff, students, and families on asthma, such as proper inhaler use and asthma signs and symptoms; and improve their own knowledge, such as being more skilled in creating health care plans for students. Practice changes also included requesting asthma action plans to ensure all students with asthma had an asthma action plan on file, standardizing asthma action plans, or modifying care plans to be in accordance with performance standards. School nurses described changes made to ensure students had access to inhalers at school and during school-related events, as well as encouraging spacer use and following up with students after rescue inhaler use. School nurses reported advocating for self-carrying medications in their school, ensuring staff were aware of students who self-carry medications, or sharing asthma action plans with teachers to allow students to safely self-carry medications; 1 respondent described asking students who self-carry medications to demonstrate proper inhaler use. Other practice changes related to completing asthma assessments, providing support for asthma trigger reduction, collecting data, checking oxygen saturation regularly, and encouraging medical provider visits. When school nurses were asked to describe their biggest challenge to implementing the standards for asthma care in school, of the 97 participants who used the toolkit, 57 (59%) provided a brief description of challenges. Time (eg, being busy), parents (eg, parental involvement, communication, support, obtaining asthma action plans), support (eg, staff compliance, administrator buy-in, physician response, being understaffed), and being able to identify students with asthma were reported challenges. Of the 43 respondents who did not use the toolkit, 22 (51%) briefly described challenges as time, parents (eg, parental involvement, communication, cooperation, support), and communication and collaboration. We aimed to identify the types of practice changes made as a result of toolkit use. Our findings suggest the toolkit reinforced practices for training of staff on the tier levels for asthma management and emergency response training and with educating staff, students, and families on asthma and proper use of asthma medications. School nurses also reported standardizing asthma action plans, increasing the number of students’ asthma action plans on file, and advocating for self-carry of asthma medications in schools. Some school nurses improved their own skills with recording asthma episodes and developing care plans. We gained a limited understanding of challenges encountered by school nurses when implementing the standards of care for asthma; these challenges were noted in previous research (7,13). Introducing a model for school nurse–led management can help schools meet the health needs of students with asthma, especially those with multiple and complex barriers to health and academic success, and provide professional support for school nurses to moderate challenges (14). Evaluation findings confirmed that our promotional efforts prompted school nurses to access the toolkit. School nurses reported using the toolkit, and the uptick in web page visits and time on page generally corresponded with promotional activities. Replication of this approach could be used to promote additional toolkits developed for school nurses to support students with other health conditions. Our study has several limitations. Findings are not generalizable to all school nurses due to low response rates. Additionally, survey and Kahoot! respondents were reached through the SSNC’s newsletter and a Michigan Association of School Nurses conference and may not reflect the entire population of school nurses. A school nurse could have participated in the survey and Kahoot! and may be represented more than once. We did not collect information on demographic characteristics of school nurses in Michigan. Practice changes were based on self-report and could not be externally validated, and our understanding of aspects of the toolkit that school nurses deemed most useful was limited. Additionally, the scope of the evaluation did not examine whether practice changes led to improved asthma outcomes for students. This project was supported by the funding opportunity CDC-RFA-EH19-1902, “A Comprehensive Public Health Approach to Asthma Control through Evidence-Based Interventions,” cooperative agreement NUE1EH001380, from the Centers for Disease Control and Prevention (CDC) to the MDHHS. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of CDC or MDHHS. Use of trade names is for identification only and does not imply endorsement by CDC, the Public Health Service, or the US Department of Health and Human Services. The authors declared no potential conflicts of interest with respect to the research, authorship, or publication of this article. No copyrighted material, surveys, instruments, or tools were used in the research described in this article. Corresponding Author: John Dowling, MA, Asthma Prevention and Control Program, Michigan Department of Health and Human Services, PO Box 30195, Lansing, MI 48909 ( [email protected] ). Author Affiliations: 1 Wingspan Research Group, Grand Rapids, Michigan. 2 Michigan Department of Education, Lansing, Michigan. 3 Asthma Prevention and Control Program, Michigan Department of Health and Human Services, Lansing, Michigan.
The opinions expressed by authors contributing to this journal do not necessarily reflect the opinions of the U.S. Department of Health and Human Services, the Public Health Service, the Centers for Disease Control and Prevention, or the authors’ affiliated institutions. |
IMAGES
COMMENTS
Nursing Diagnosis. Based on the data gathered, the nursing diagnoses appropriate for the patient with asthma include: Ineffective airway clearance related to increased production of mucus and bronchospasm. Impaired gas exchange related to altered delivery of inspired O2. Anxiety related to perceived threat of death.
The majority of adverse effects occurred within 1 day of the procedure and resolved within 7 days. 6. In this study, bronchial thermoplasty was found to significantly improve quality of life, as ...
Hey everyone. My name is Abby. We're going to cover a case study today about pediatric asthma. Let's get started. Anthony is a six year old male patient brought to the ER with a history of asthma. Since he came home from the NICU as an infant, he has lived with his parents, Bob and Josh, who adopted him after fostering him from the age of four ...
The case study presented here is reported separately because it provides an exemplar of nursing leading integrated whole-system service provision for children with asthma. Background The growth of networked and partnership collaborations arises from the recognition that a number of the most pressing public health problems cannot be addressed by ...
Supported self-management reduces asthma morbidity. The lady in this case study is struggling to maintain control of her asthma within the context of her busy professional and domestic life.
Schools with limited nursing services can establish a system to maintain the administration of preventive asthma medications as seen in Halterman et al.'s (2018) study, where an asthma care coordinator who received additional asthma training was appointed to assist the school nurse in communicating with the physician, families, and school ...
Moreover, in a real-life study of 104 children and adolescents with severe allergic refractory asthma followed over 1 year, treatment with omalizumab resulted in good asthma control in 67% of the cases (p < 0.001), while FEV 1 improved by 4.9% (p = 0.02) and exacerbation rates and healthcare utilisation decreased approximately by 30% (p < 0.001) .
Purpose: To review the pathophysiology of asthma, present a case study, and provide management strategies for treating this common, yet complex disorder in children and adults. Data sources: Selected clinical guidelines, clinical articles, and research studies. Conclusions: Asthma is a chronic inflammatory airway disorder with acute exacerbations that currently affects approximately 14 million ...
CASE REPORT. In January 2020, a 53-year-old gentleman with a background of asthma on long-term low dose inhaled corticosteroid inhaler had an acute exacerbation of his asthma in February 2020 triggered by a viral upper respiratory tract infection and acute sinusitis and was managed with bronchodilator nebulization and a 7-day course of oral prednisone 30 mg daily.
Method: A mixed-method single-case study design using Yin's approach, including focus groups, interviews, and analysis of policy documents and public health reports. Results: A model that explains the integrated population approach to managing school-age asthma is described; the role of the lead school nurse coordinator was seen as critical to ...
Asthma Case Study. Asthma affects about 6.1 million children in the US under 18 years of age, making it one of the most common chronic childhood disorders (American Lung Association, 2021). Asthma occurs as a result of a stimulus which can range from allergens, cigarette smoke, changes in temperature, stress, or exercise. ...
In recent years, it has gained increasing notoriety in schools and in the media. Population-based studies have shown that 20% to 35% of children with allergies experience bullying. In many cases (31% in one recent study ), this bullying is related directly to the food allergy. From a medical perspective, there are little published data ...
Aim To describe the role of school nursing in leading and coordinating a multidisciplinary networked system of support for children with asthma, and to analyze the strengths and challenges of ...
Asthma is a complex disease that involves physiological, environmental, and psychosocial factors. This paper reviews childhood asthma case management by social service professionals, lay health workers, and nurses, and it presents a new randomized controlled study using nurse case management in a local community coalition. Evidence suggests the common factor for success involves case managers ...
The International Primary Care Respiratory Group is a Scottish Charity (SC 035056) and a Scottish Company Limited by guarantee (Scottish Company Number 256268). Registered office: 4th Floor, 115 George Street, Edinburgh, Scotland, EH2 4JN.
UNFOLDING Reasoning Case Study: STUDENT Pediatric Asthma History of Present Problem: Jared Johnson is a 10 year-old African-American boy with a history of moderate persistent asthma. He is being admitted to the pediatric unit of the hospital from the walk-in clinic with an acute asthma exacerbation.
Summary. This chapter presents a case study of a 10-year-old girl with moderate intermittent asthma diagnosed at age 4 and was admitted to the pediatric intensive care unit with status asthmaticus. The case study includes details about history of present illness, past medical history, past surgical history, family history, and current status.
Case study about asthma in patients that are specifically pediatric. case study 105 asthma is who has been brought to the emergency department (ed) his mother. ... Identify the nursing responsibilities associated with giving albuterol Assess for hypersensitivity, assess lung sounds pulse and blood pressure, tell L to report any adverse effects. ...
Asthma Scenario 1. 9 year old Alan comes in with complaints of "chest tightness". His breathing is mildly labored and he is audibly wheezing. His peak flow is 50% of his normal range. Significant findings include moderate inspiratory and expiratory wheezing with moderate air exchange. His O2 is 96% by pulse oximetry.
16. Keith RN Congenital Heart Disease Case Study. Pediatrics Nursing Lab93%(15) 1. Newborn hypoglycemia - 5evib7uynijlijk kuyvkuyblkjn ghrdvtfbygnulilnikuybtfvtbyn kjyvdcrtyrbitnum tybunlmoiyutf. Pediatrics Nursing Lab92%(13) Nur 211 pediatric asthma unfolding reasoning jared johnson, 10 years old primary concept gas exchange interrelated ...
Study with Quizlet and memorize flashcards containing terms like Meet the Client: Joshua MartinJoshua Martin is a 5-year-old boy who started kindergarten this year. The school nurse notices that Joshua has a persistent dry cough, wheezing, and difficulty keeping up with the other children on the playground. Joshua's wheezing intensifies after he lies on the floor mats in his classroom for a ...
The case study presented here is reported separately because it provides an exemplar of nursing leading integrated whole-system service provision for children with asthma. Background The growth of networked and partnership collaborations arises from the recognition that a number of the most pressing public health problems cannot be addressed by ...
Nursing diagnosis: Impaired gas exchange r/t mismatch of ventilation and perfusion aeb O 90%, R- 24, pCO2 - 46. Subjective/objective assessment data: Client says she hasn't taken her asthma medication in past 2 days; working hard to breathe as she speaks; SOB; O 90%, pCO2 - 46 (Vera, 2012) (Taylor, Lynn, & Bartlett, 2019, p. 1488, 1497, 1499)
In the context of this case-control study, the presence of symptoms related to asthma and rhinitis was assessed using the Brazilian version of the International Study of Asthma and Allergies in Childhood (ISAAC) questionnaire [17,18,19]. Although the ISAAC is widely recognized and validated for assessing the prevalence and severity of allergic ...
From 2017 to 2021, 18.4% of Michigan children and adolescents aged 5 to 17 years with current asthma had an asthma-related visit to an emergency department or urgent care in the past 12 months; however, 30.9% of Black children and adolescents and 26.0% of children and adolescents in households with less than $50,000 in annual income had an ...